Influence of the Maxillary Sinus on the Accuracy of the Root ZX Apex Locator: An Ex Vivo Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Teeth
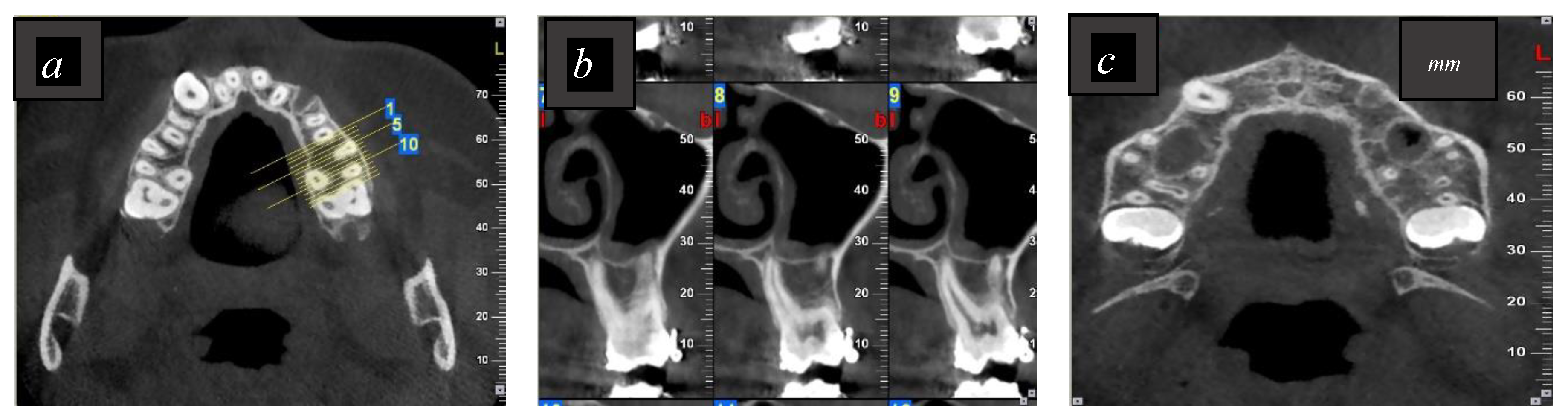
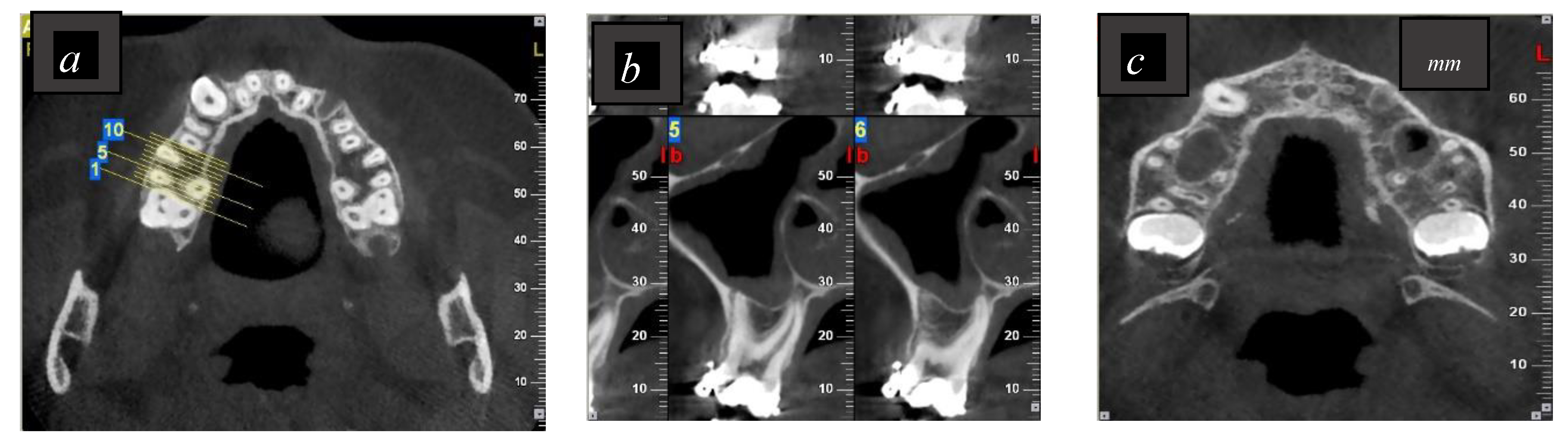
2.2. Imaging Procedures and Evaluation of the CBCT Images
2.3. Determination of the Electronic Working Length Using Root ZX
2.4. Determination of the Real Working Length Using a Glass Plate
2.5. Statistical Analyses
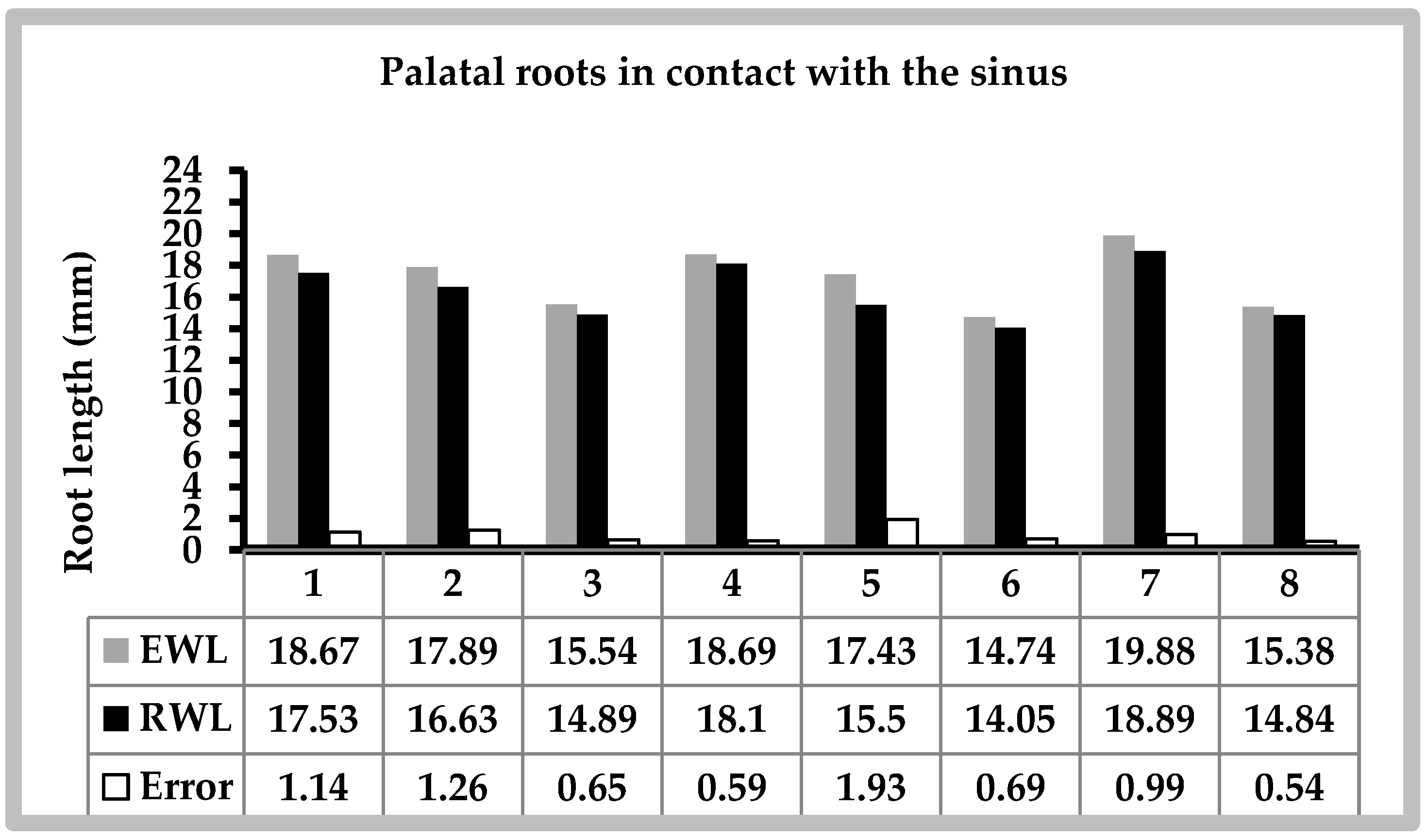
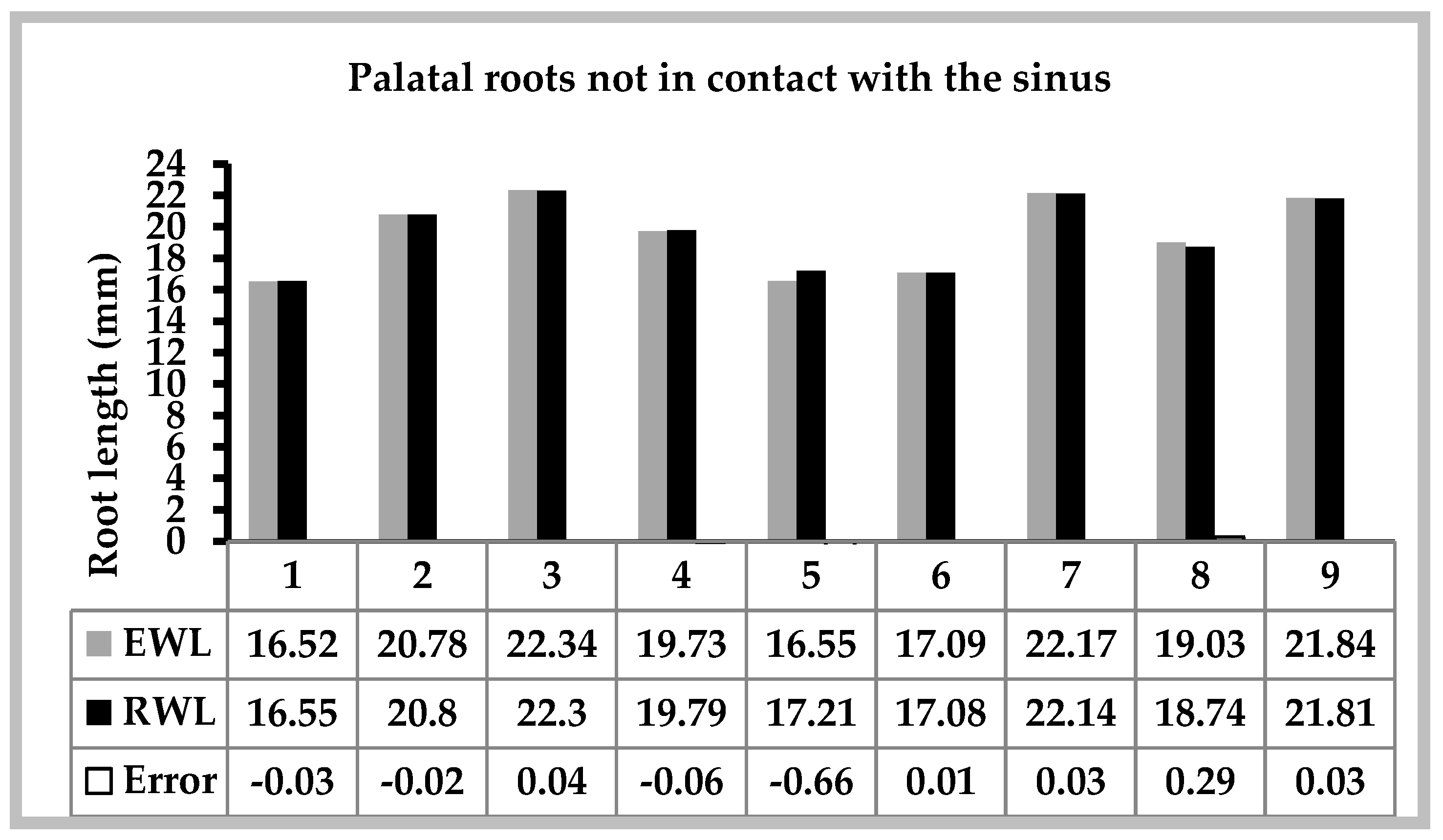
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siqueira, J.F., Jr.; Rocas, I.N. Distinctive features of the microbiota associated with different forms of apical periodontitis. J. Oral Microbiol. 2009, 1. [Google Scholar] [CrossRef]
- ElAyouti, A.; Hülber, J.M.; Judenhofer, M.S.; Connert, T.; Mannheim, J.G.; Löst, C.; Pichler, B.J.; von Ohle, C. Apical constriction: Location and dimensions in molars—A micro–computed tomography study. J. Endod. 2014, 40, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, M.A.; White, R.R.; Walton, R.E. Determining the optimal obturation length: A meta-analysis of literature. J. Endod. 2005, 31, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D. Apical limit of root canal instrumentation and obturation, part 1. Literature review. Int. Endod. J. 1998, 31, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Sjogren, U.; Hagglund, B.; Sundqvist, G.; Wing, K. Factors affecting the long-term results of endodontic treatment. J. Endod. 1990, 16, 498–504. [Google Scholar] [CrossRef]
- Fouad, A.F.; Reid, L.C. Effect of using electronic apex locators on selected endodontic treatment parameters. J. Endod. 2000, 26, 364–367. [Google Scholar] [CrossRef] [PubMed]
- De Morais, A.L.; de Alencar, A.H.; Estrela, C.R.; Decurcio, D.A.; Estrela, C. Working Length Determination Using Cone-Beam Computed Tomography, Periapical Radiography and Electronic Apex Locator in Teeth with Apical Periodontitis: A Clinical Study. Iran. Endod. J. 2016, 1, 164–168. [Google Scholar]
- Akisue, E.; Gratieri, S.D.; Barletta, F.B.; Caldeira, C.L.; Grazziotin-Soares, R.; Gavini, G. Not all electronic foramen locators are accurate in teeth with enlarged apical foramina: An in vitro comparison of 5 brands. J. Endod. 2014, 40, 109–112. [Google Scholar] [CrossRef]
- Martins, J.N.; Marques, D.; Mata, A.; Carames, J. Clinical efficacy of electronic apex locators: Systematic review. J. Endod. 2014. [Google Scholar] [CrossRef]
- Nekoofar, M.H.; Ghandhi, M.; Hayes, S.J.; Dummer, P.M.H. The fundamental operating principles of electronic root canal length measurement devices. Int. Endod. J. 2006, 39, 595–609. [Google Scholar] [CrossRef]
- Venturi, M.; Breschi, L. A comparison between two electronic apex locators: An in vivo investigation. Int. Endod. J. 2005, 38, 36–45. [Google Scholar] [CrossRef] [PubMed]
- D’Assunção, F.L.; de Albuquerque, D.S.; Salazar-Silva, J.R.; de Queiroz Ferreira, L.C.; Bezerra, P.M. The accuracy of root canal measurements using the Mini Apex Locator and Root ZX-II: An evaluation in vitro. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 104, E50–E53. [Google Scholar] [CrossRef] [PubMed]
- Wrbas, K.T.; Ziegler, A.A.; Altenburger, M.J.; Schirrmeister, J.F. In vivo comparison of working length determination with two electronic apex locators. Int. Endod. J. 2007, 40, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Saatchi, M.; Iravani, S.; Iravani Khaleghi, M.; Mortaheb, A. Influence of Root Canal Curvature on the Accuracy of of Root ZX Electronic Foramen Locator: An in Vitro Study. Iran. Endod. J. 2017, 12, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; Felici, R.; Conte, G.; Costantini, M.; Cianconi, L. Accuracy of three electronic apex locators in anterior and posterior teeth: An ex vivo study. J. Endod. 2011, 37, 684–687. [Google Scholar] [CrossRef] [PubMed]
- Herrera, M.; Abalos, C.; Lucena, C.; Jiménez-Planas, A.; Llamas, R. Critical diameter of apical foramen and of file size using the Root ZX apex locator: An in vitro study. J. Endod. 2011, 37, 1306–1309. [Google Scholar] [CrossRef] [PubMed]
- Akisue, E.; Gavini, G.; de Figueiredo, J.A. Influence of pulp vitality on length determination by using the Elements Diagnostic Unit and Apex Locator. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 104, 129–132. [Google Scholar] [CrossRef]
- Prasad, A.B.; Harshit, S.; Aastha, S.A.; Deepak, R. An In vitro Evaluation of the Accuracy of Two Electronic Apex Locators to Determine Working Length in the Presence of Various Irrigants. Ethiop. J. Health Sci. 2016, 26, 457–462. [Google Scholar] [CrossRef]
- Nazari Moghaddam, K.; Nazari, S.; Shakeri, L.; Honardar, K.; Mirmotalebi, F. In vitro detection of simulated apical root perforation with two electronic apex locators. Iran. Endod. J. 2010, 5, 23–26. [Google Scholar]
- Piasecki, L.; Carneiro, E.U.; Neto Westphalen, V.; Brandao, C.; Gambarini, G.; Azim, A. The use of micro computed tomography to determine the accuracy of 2 electronic apex locators and anatomic variations affecting their precision. J. Endod. 2016, 42, 1263–1267. [Google Scholar] [CrossRef]
- Gu, Y.; Sun, C.; Wu, D.; Zhu, Q.; Leng, D.; Zhou, Y. Evaluation of the relationship between maxillary posterior teeth and the maxillary sinus floor using cone-beam computed tomography. BMC Oral Health 2018, 18, 164. [Google Scholar] [CrossRef] [PubMed]
- Maridati, P.; Stoffella, E.; Speroni, S.; Cicciu, M.; Maiorana, C. Alveolar Antral Artery Isolation during Sinus Lift Procedure with the Double Window Technique. Open Dent. J. 2014, 8, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Beretta, M.; Cicciu, M.; Bramanti, E.; Maiorana, C. Schneider membrane elevation in presence of sinus septa: Anatomic features and surgical management. Int. J. Dent. 2012, 261905. [Google Scholar] [CrossRef] [PubMed]
- Hauman, C.H.; Chandler, N.P.; Tong, D.C. Endodontic implications of the maxillary sinus: A review. Int. Endod. J. 2002, 35, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Ikeda, T.; Yokoi, H.; Kohno, N. Association between odontogenic infections and unilateral sinus opacification. Auris Nasus Larynx 2015, 42, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Roque-Torres, G.D.; Ramirez-Sotelo, L.R.; Vaz, S.L.D.A.; Bóscolo, S.M.D.A.D.; Bóscolo, F.N. Association between maxillary sinus pathologies and healthy teeth. Braz. J. Otorhinolaryngol. 2016, 82, 33–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khongkhunthian, P.; Reichart, P.A. Aspergillosis of the maxillary sinus as a complication of overfilling root canal material into the sinus: Report of two cases. J. Endod. 2001, 27, 476–478. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Cho, K.M.; Park, S.H.; Park, S.R.; Lee, S.S.; Lee, S.K. Chronic maxillary sinusitis caused by root canal overfilling of Calcipex II. Restor. Dent. Endod. 2014, 39, 63–67. [Google Scholar] [CrossRef]
- Patel, S.; Dawood, A.; Ford, T.P.; Whaites, E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int. Endod. J. 2007, 40, 818–830. [Google Scholar] [CrossRef]
- Nair, M.K.; Nair, U.P. Digital and advanced imaging in endodontics: A review. J. Endod. 2007, 33, 1–6. [Google Scholar] [CrossRef]
- Demirbuga, S.; Sekerci, A.E.; Dincer, A.N.; Cayabatmaz, M.; Zorba, Y.O. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular first and second molars in Turkish individuals. Med. Oral Patol. Oral Cir. Bucal 2013, 18, 737–744. [Google Scholar] [CrossRef]
- Rancitelli, D.; Borgonovo, A.E.; Cicciù, M.; Re, D.; Rizza, F.; Frigo, A.C.; Maiorana, C. Maxilary sinus Septa and Anatomic Correlation with the Schneideerian Membrane. J. Craniofac. Surg. 2015, 26, 1394–1398. [Google Scholar] [CrossRef] [PubMed]
- Ozer, S.Y. Detection of vertical root fractures of different thicknesses in endodontically enlarged teeth by cone beam computed tomography versus digital radiography. J. Endod. 2010, 36, 1245–1249. [Google Scholar] [CrossRef] [PubMed]
- Cotton, T.P.; Geisler, T.M.; Holden, D.T.; Schwartz, S.A.; Schindler, W.G. Endodontic applications of cone-beam volumetric tomography. J. Endod. 2007, 33, 1121–1132. [Google Scholar] [CrossRef] [PubMed]
- Laino, L.; Troiano, G.; Giannatempo, G.; Graziani, U.; Ciavarella, D.; Dioguardi, M.; Lo Muzio, L.; Lauritano, F.; Cicciù, M. Sinus Lift Augmentation by Using Calcium Sulphate. A Retrospective 12 Months Radiographic Evaluation Over 25 Treated Italian Patients. Open Dent. J. 2015, 22, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Kilic, C.; Kamburoglu, K.; Yuksel, S.P.; Yuksel, T. An Assessment of the Relationship between the Maxillary Sinus Floor and the Maxillary Posterior Teeth Root Tips Using Dental Cone-beam Computerized Tomography. Eur. J. Dent. 2010, 4, 462–467. [Google Scholar] [PubMed]
- Kang, S.H.; Kim, B.S.; Kim, Y. Proximity of posterior teeth to the maxillary sinus and buccal bone thickness: A biometrical assessment using cone-beam tomography. J. Endod. 2015, 41, 1839–1846. [Google Scholar] [CrossRef]
- Tian, X.M.; Qian, L.; Xin, X.Z.; Wei, B.; Gong, Y. An analysis of the proximity of maxillary posterior teeth to the maxillary sinus using cone-beam computed tomography. J. Endod. 2016, 42, 371–377. [Google Scholar] [CrossRef]
- Aksoy, U.; Orhan, K. Association between odontogenic conditions and maxillary sinus mucosal thickening: A retrospective CBCT study. Clin. Oral Investig. 2018, 1–9. [Google Scholar] [CrossRef]
- Üstün, Y.; Aslan, T.; Şekerci, A.E.; Sağsen, B. Evaluation of the reliability of cone-beam Computed Tomography scanning and Electronic Apex Locator Measurements in Working Length Determination with Large Periapical Lesions. J. Endod. 2016, 42, 1334–1337. [Google Scholar] [CrossRef]
- Kasikcioglu, A.; Gulsahi, A. Relationship between maxillarynsinus pathologies and maxillary posterior tooth periapical pathologies. Oral Radiol. 2016, 32, 180–186. [Google Scholar] [CrossRef]
- Pauwels, R.; Jacobs, R.; Bosmans, H.; Schulze, R. Future prospects for dental cone beam CT imaging. Imaging Med. 2012, 4, 551–563. [Google Scholar] [CrossRef]
- Scarfe, W.C.; Li, Z.; Aboelmaaty, W.; Scott, S.A.; Farman, A.G. Maxillofacial cone beam computed tomography: Essence, elements and steps to interpretation. Aust. Dent. J. 2012, 57 (Suppl. 1), 46–60. [Google Scholar] [CrossRef]
- Angelopoulos, C.; Scarfe, W.C.; Farman, A.G. A comparison of maxillofacial CBCT and medical CT. Atlas Oral Maxillofac. Surg. Clin. North. Am. 2012, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, F.; Kamburoğlu, K.; Şenel, B. Endodontic working length measurement using cone-beam computed tomographic images obtained at different voxel sizes and field of views, periapical radiography, and apex locator: A comparative ex vivo study. J. Endod. 2017, 43, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Haupt, F.; Hülsmann, M. Consistency of electronic measurements of endodontic working length when using multiple devices from the same manufacturer-an in vitro study. Clin. Oral Investig. 2018. [CrossRef] [PubMed]
- Baruah, Q.; Sinha, N.; Singh, B.; Reddy, P.N.; Baruah, K.; Augustine, V. Comparative Evaluation of Accuracy of Two Electronic Apex Locators in the Presence of Contemporary Irrigants: An In vitro Study. J. Int. Soc. Prev. Community Dent. 2018, 8, 349–353. [Google Scholar] [CrossRef]
- Oliveira, T.N.; Vivacqua-Gomes, N.; Bernardes, R.A.; Vivan, R.R.; Duarte, M.A.H.; Vasconcelos, B.C. Determination of the Accuracy of 5 Electronic Apex Locators in the Function of Different Employment Protocols. J. Endod. 2017, 10, 1663–1667. [Google Scholar] [CrossRef]
- Camargo, E.J.; Zapata, R.O.; Mederos, P.L.; Bramante, C.M.; Bernardineli, N.; Garcia, R.B.; de Moraes, I.G.; Duarte, M.A. Influence of preflaring on the Accuracy of Length Determination with Four Electronic apex locators. J. Endod. 2009, 35, 1300–1302. [Google Scholar] [CrossRef]
- ElAyouti, A.; Dima, E.; Ohmer, J.; Sperl, K.; von Ohle, C.; Löst, C. Consistency of apex locator function: A clinical study. J. Endod. 2009, 35, 179–181. [Google Scholar] [CrossRef]
- Tsesis, I.; Blazer, T.; Taschieri, G.; Fabbro, M.; Corbella, S.; Rosen, E. The precision in electronic apex locators in electronic working length determination: A systematic review and meta-analysis of the literature. J. Endod. 2015, 4, 1818–1823. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, C.; Suda, H. New electronic canal measuring device based on the ratio method. J. Endod. 1994, 20, 111–114. [Google Scholar] [CrossRef]
- Nguyen, H.Q.; Kaufman, A.Y.; Komorowski, R.C.; Friedman, S. Electronic length measurement using small and large files in enlarged canals. Int. Endod. J. 1996, 29, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Azabal, M.D.; Garcia-Otero, D.; De la Macorra, J.C. Accuracy of the Justy II Apex locator in determining working length in simulated horizontal and vertical fractures. Int. Endod. J. 2004, 37, 174–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandewal, D.; Ballal, N.; Saraswathi, M. Comparative evaluation of accuracy of 2 electronic apex locators with conventional radiography: An ex vivo study. J. Endod. 2015, 41, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.A. Transantral endodontic surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1996, 82, 80–83. [Google Scholar]
- De Vasconcelos, B.C.; Do Vale, T.M.; De Menezes, A.S.; Pinheiro-Junior, E.C.; Vivacqua-Gomes, N.; Bernardes, R.A.; Hungaro Duarte, M.A. An ex vivo comparison of root canal length determination by three electronic apex locators at positions short of the apical foramen. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 11, 57–61. [Google Scholar] [CrossRef]
- Aguiar, B.A.; Reinaldo, R.S.; Frota, L.M.A.; do Vale, M.S.; Vasconcelos, B.C.D. Root ZX Electronic Foramen Locator: An Ex Vivo Study of Its Three Models’ Precision and Reproducibility. Int. J. Dent. 2017, 5893790. [Google Scholar] [CrossRef] [PubMed]
- ElAyouti, A.; Weiger, R.; Löst, C. The ability of root ZX apex locator to reduce the frequency of overestimated radiographic working length. J. Endod. 2002, 28, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Ericson, S.; Finne, K.; Persson, G. Results of apicoectomy of maxillary canines, premolars and molars with special reference to oroantral communication as a prognostic factor. Int. J. Oral Surg. 1974, 3, 386–393. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Gutmann, J.L. Factors associated with postobturation pain following single-visit nonsurgical root canal treatment: A systematic review. Quintessence Int. 2017, 48, 193–208. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.P.; Chandler, N.P. Electronic apex locators: A review. Int. Endod. J. 2004, 37, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Neelakantan, P. Endodontic Microbiology—A Special Issue of Dentistry Journal. Dent. J. (Basel) 2018, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Jung, I.Y.; Yoon, B.H.; Lee, S.J.; Lee, S.J. Comparison of the reliability of “0.5” and “APEX” mark measurements in two frequency-based electronic apex locators. J. Endod. 2011, 37, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Segato, A.V.K.; Piasecki, L.; Felipe Iparraguirre Nuñovero, M.; da Silva Neto, UX.; Westphalen, V.P.D.; Gambarini, G.; Carneiro, E. The Accuracy of a New Cone-beam Computed Tomographic Software in the Preoperative Working Length Determination Ex Vivo. J. Endod. 2018, 44, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- Zand, V.; Rahimi, S.; Davoudi, P.; Afshang, A. Accuracy of Working Length Determination using NovApex and Root-ZX Apex Locators: An in vitro Study. J. Contemp. Dent. Pract. 2017, 18, 383–385. [Google Scholar] [CrossRef] [PubMed]
- Shabahang, S.; Goon, W.W.; Gluskin, A.H. An in vivo evaluation of Root ZX electronic apex locator. J. Endod. 1996, 22, 616–618. [Google Scholar] [CrossRef]
- Tselnik, M.; Baumgartner, J.C.; Marshall, J.G. An evaluation of root ZX and elements diagnostic apex locators. J. Endod. 2005, 31, 507–509. [Google Scholar] [CrossRef]
- Plotino, G.; Grande, N.M.; Brigante, L.; Lesti, B.; Somma, F. Ex vivo accuracy of three electronic apex locators: Root ZX, Elements Diagnostic Unit and Apex Locator and ProPex. Int. Endod. J. 2006, 39, 408–414. [Google Scholar] [CrossRef]
- Jenkins, J.A.; Walker, W.A.; Schindler, W.G.; Flores, C.M. An in vitro evaluation of the accuracy of the root ZX in the presence of various irrigants. J. Endod. 2001, 27, 209–211. [Google Scholar] [CrossRef]
- Alothmani, O.S. The accuracy of Root ZX electronic apex locator. Saudi Endod. J. 2012, 2, 11530. [Google Scholar] [CrossRef]
- Ding, J.; Gutmann, J.L.; Fan, B.; Lu, Y.; Chen, H. Investigation of apex locators and related morphological factors. J. Endod. 2010, 36, 1399–1403. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, A.K.; Yoshioka, T.; Kobayashi, C.; Suda, H. The effects of file size, sodium hypochlorite and blood on the accuracy of Root ZX apex locator in enlarged root canals: An in vitro study. Aust. Dent. J. 2006, 51, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Haffner, C.; Folwaczny, M.; Galler, K.; Hickel, R. Accuracy of electronic apex locators in comparison to actual length—An in vivo study. J. Dent. 2005, 33, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Duran-Sindreu, F.; Gomes, S.; Stober, E.; Mercade, M.; Jane, L.; Roig, M. In vivo evaluation of the iPex and Root ZX electronic apex locators using various irrigants. Int. Endod. J. 2013, 46, 769–774. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Mean RWL (mm) | Mean EWL (mm) | Mean Error |
|---|---|---|---|
| Roots in contact with the sinus (n = 8) | 16.304 ± 1.748 | 17.278 ± 1.858 | +0.974 ± 0.470 |
| Roots not in contact with the sinus (n = 9) | 19.602 ± 2.297 | 19.561 ± 2.396 | −0.041 ± 0.253 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Hachem, R.; Wassef, E.; Mokbel, N.; Abboud, R.; Zogheib, C.; El Osta, N.; Naaman, A. Influence of the Maxillary Sinus on the Accuracy of the Root ZX Apex Locator: An Ex Vivo Study. Dent. J. 2019, 7, 3. https://doi.org/10.3390/dj7010003
El Hachem R, Wassef E, Mokbel N, Abboud R, Zogheib C, El Osta N, Naaman A. Influence of the Maxillary Sinus on the Accuracy of the Root ZX Apex Locator: An Ex Vivo Study. Dentistry Journal. 2019; 7(1):3. https://doi.org/10.3390/dj7010003
Chicago/Turabian StyleEl Hachem, Roula, Elie Wassef, Nadim Mokbel, Richard Abboud, Carla Zogheib, Nada El Osta, and Alfred Naaman. 2019. "Influence of the Maxillary Sinus on the Accuracy of the Root ZX Apex Locator: An Ex Vivo Study" Dentistry Journal 7, no. 1: 3. https://doi.org/10.3390/dj7010003