Tumor Location Influences Oncologic Outcomes of Hepatocellular Carcinoma Patients Undergoing Radiofrequency Ablation

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Operation Success and Complications
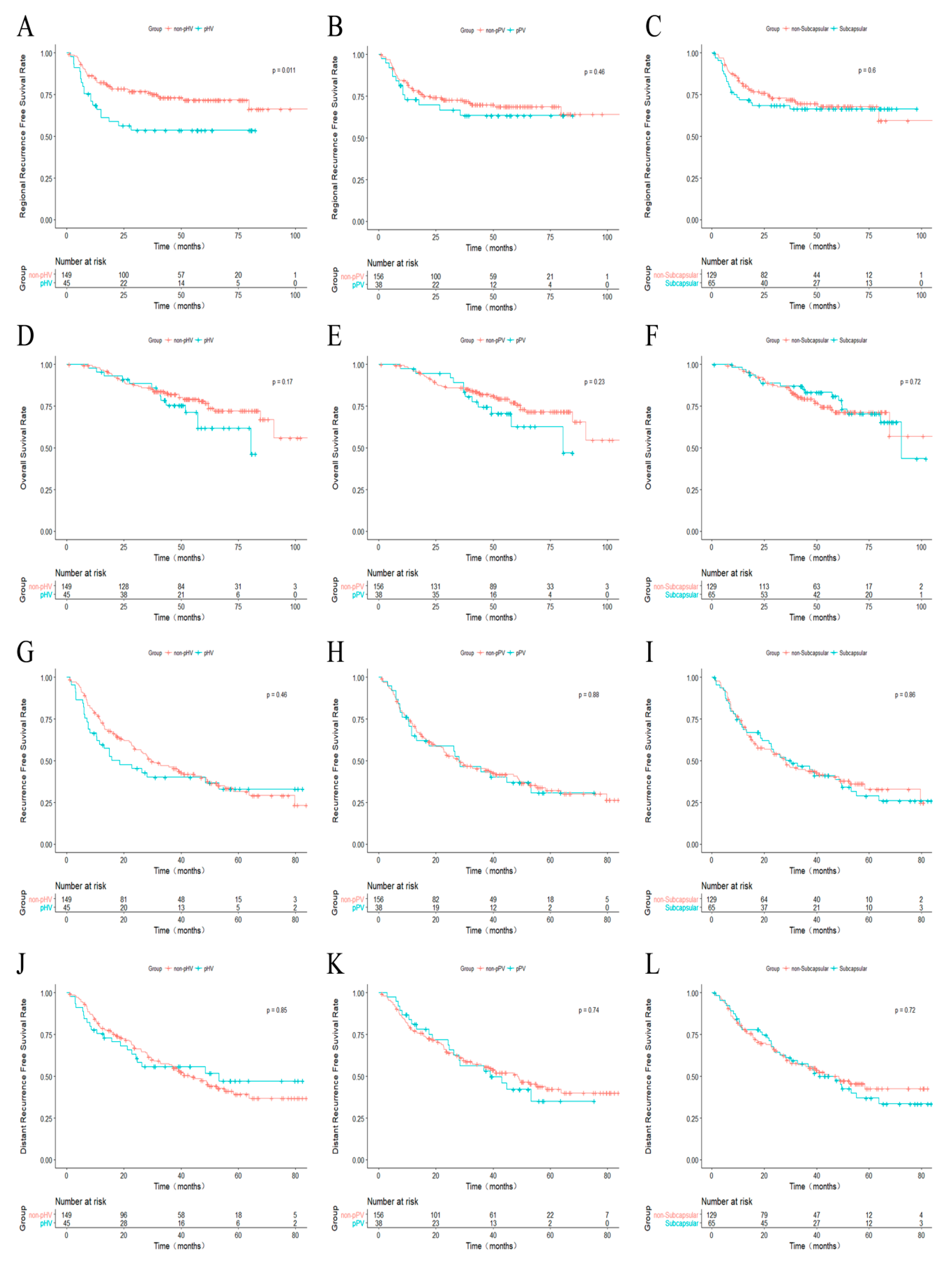
2.3. Recurrence and Survival Outcomes
2.4. Univariate and Multivariate Analysis
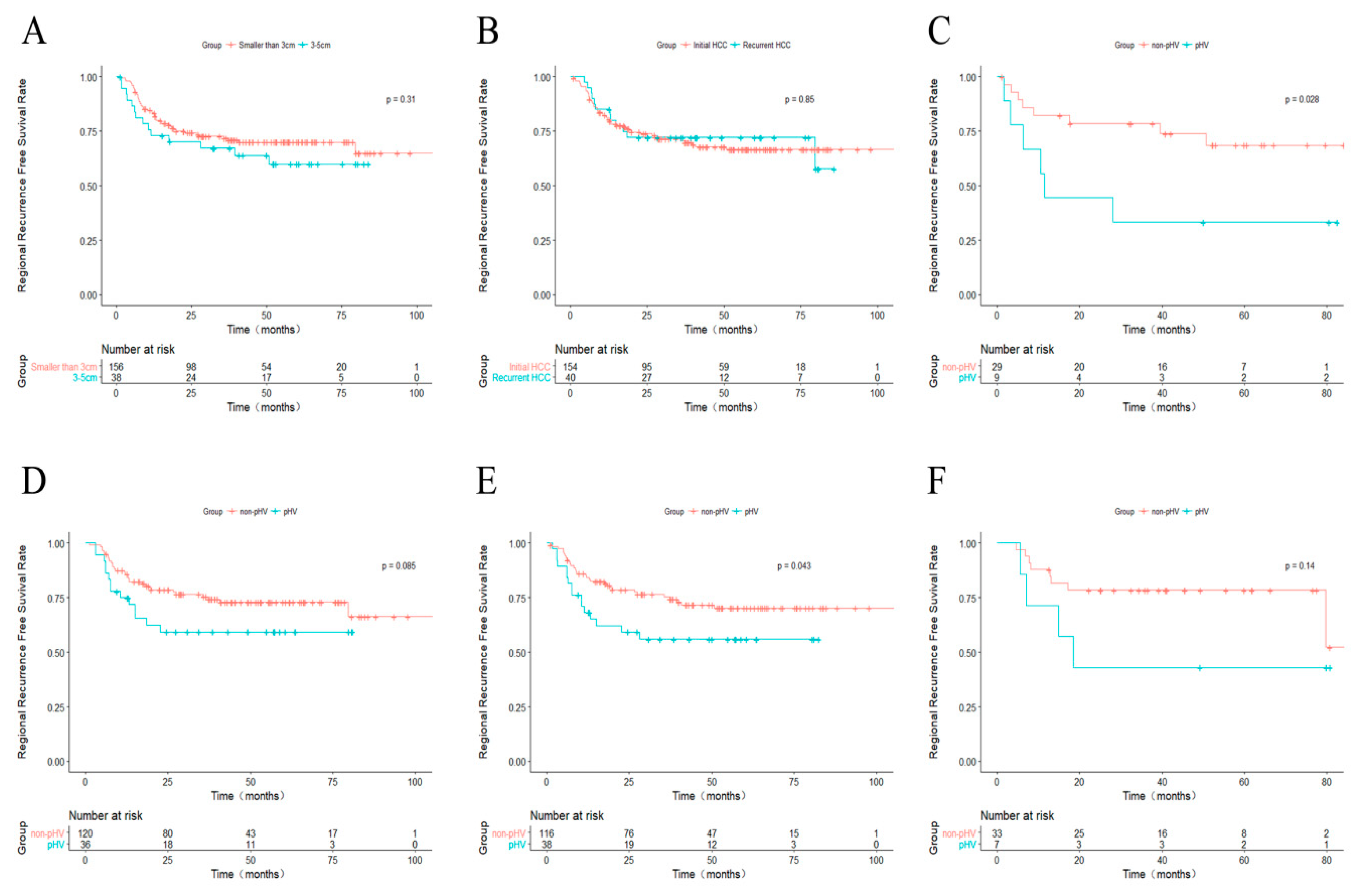
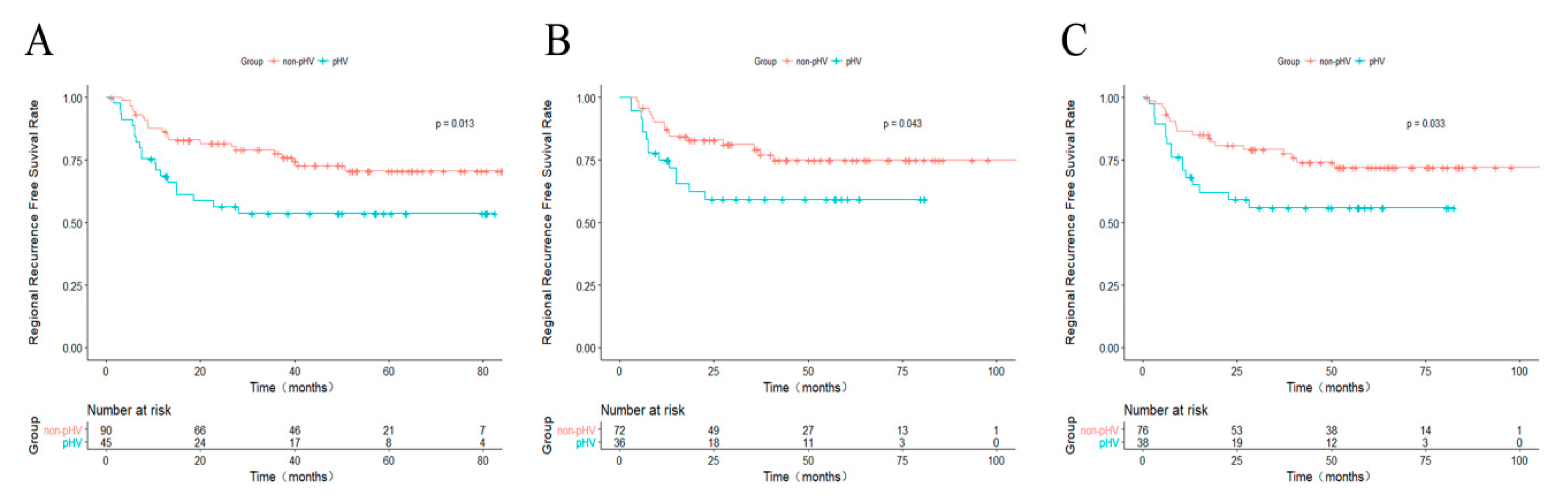
2.5. Further Analysis for pHV and Non-pHV HCCs
3. Discussion
4. Materials and Methods
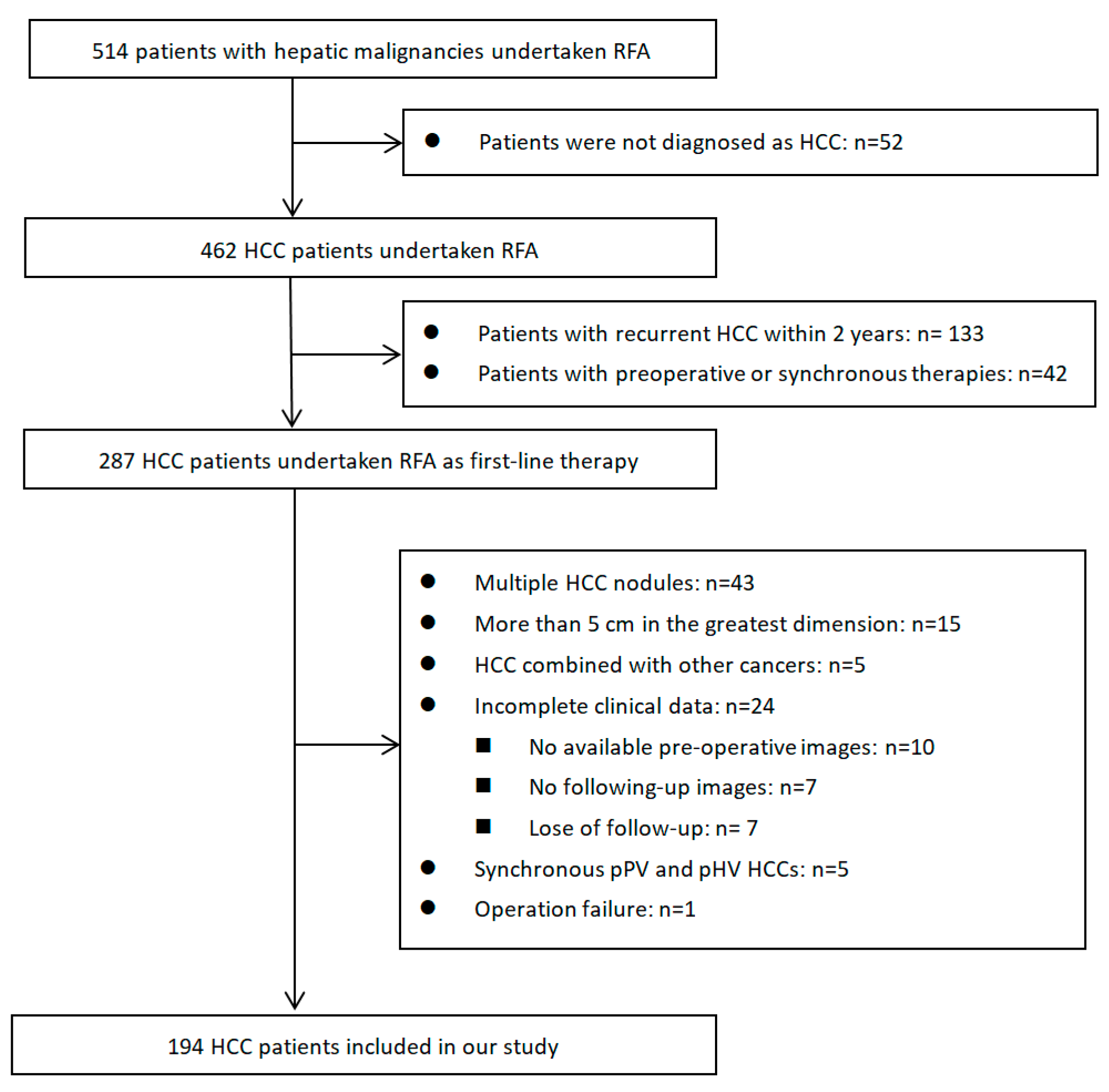
4.1. Study Population and Design
4.2. Definition of Perivascular HCC and Subcapsular HCC
4.3. RFA Procedure
4.4. Following Up
4.5. Outcomes
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.S.; Li, J.Q.; Zheng, Y.; Guo, R.P.; Liang, H.H.; Zhang, Y.Q.; Lin, X.J.; Lau, W.Y. A prospective randomized trial comparing percutaneous local ablative therapy and partial hepatectomy for small hepatocellular carcinoma. Ann. Surg. 2006, 243, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.E.; De Lope, C.R.; Bruix, J. Current strategy for staging and treatment: The bclc update and future prospects. Semin. Liver Dis. 2010, 30, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Hocquelet, A.; Balageas, P.; Laurent, C.; Blanc, J.F.; Frulio, N.; Salut, C.; Cassinotto, C.; Saric, J.; Possenti, L.; Bernard, P.H.; et al. Radiofrequency ablation versus surgical resection for hepatocellular carcinoma within the milan criteria: A study of 281 western patients. Int. J. Hyperth. 2015, 31, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.S.K.; Raman, S.S.; Limanond, P.; Aziz, D.; Economou, J.; Busuttil, R.; Sayre, J. Influence of large peritumoral vessels on outcome of radiofrequency ablation of liver tumors. J. Vasc. Interv. Radiol. 2003, 14, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Komorizono, Y.; Oketani, M.; Sako, K.; Yamasaki, N.; Shibatou, T.; Maeda, M.; Kohara, K.; Shigenobu, S.; Ishibashi, K.; Arima, T. Risk factors for local recurrence of small hepatocellular carcinoma tumors after a single session, single application of percutaneous radiofrequency ablation. Cancer 2003, 97, 1253–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, T.W.; Lim, H.K.; Lee, M.W.; Kim, Y.S.; Choi, D.; Rhim, H. Perivascular versus nonperivascular small hcc treated with percutaneous rf ablation: Retrospective comparison of long-term therapeutic outcomes. Radiology 2014, 270, 888–899. [Google Scholar] [CrossRef] [PubMed]
- Kang, T.W.; Lim, H.K.; Lee, M.W.; Kim, Y.S.; Rhim, H.; Lee, W.J.; Paik, Y.H.; Kim, M.J.; Ahn, J.H. Long-term therapeutic outcomes of radiofrequency ablation for subcapsular versus nonsubcapsular hepatocellular carcinoma: A propensity score matched study. Radiology 2016, 280, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Mulier, S.; Ni, Y.; Jamart, J.; Ruers, T.; Marchal, G.; Michel, L. Local recurrence after hepatic radiofrequency coagulation: Multivariate meta-analysis and review of contributing factors. Ann. Surg. 2005, 242, 158–171. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Feng, K.; Yan, J.; Li, X.; Xia, F.; Ma, K.; Wang, S.; Bie, P.; Dong, J. A randomized controlled trial of radiofrequency ablation and surgical resection in the treatment of small hepatocellular carcinoma. J. Hepatol. 2012, 57, 794–802. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.K.C.; Chok, K.S.H.; Chan, A.C.Y.; Cheung, T.T.; Wong, T.C.L.; Fung, J.Y.Y.; Yuen, J.; Poon, R.T.P.; Fan, S.T.; Lo, C.M. Randomized clinical trial of hepatic resection versus radiofrequency ablation for early-stage hepatocellular carcinoma. Br. J. Surg. 2017, 104, 1775–1784. [Google Scholar] [CrossRef] [PubMed]
- Kang, T.W.; Lim, H.K.; Cha, D.I. Aggressive tumor recurrence after radiofrequency ablation for hepatocellular carcinoma. Clin. Mol. Hepatol. 2017, 23, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.A.; Shim, J.H.; Kim, M.J.; Kim, S.Y.; Won, H.J.; Shin, Y.M.; Kim, P.N.; Kim, K.H.; Lee, S.G.; Lee, H.C. Radiofrequency ablation as an alternative to hepatic resection for single small hepatocellular carcinomas. Br. J. Surg. 2016, 103, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Wu, J.; Liu, X.; Liang, M.; Zhou, X.; Ouyang, S.; Yao, J.; Wang, J.; Luo, B. Insufficient radiofrequency ablation promotes proliferation of residual hepatocellular carcinoma via autophagy. Cancer Lett. 2018, 421, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.H.; Chen, M.S.; Zhang, Y.Q.; Guo, R.P.; Li, G.H. Experimental study on optimal operating parameters setting of radiofrequency thermal ablation in normal ex-swine livers. Ai zheng = Aizheng = Chin. J. Cancer 2005, 24, 12–18. [Google Scholar]
- Loriaud, A.; Denys, A.; Seror, O.; Vietti Violi, N.; Digklia, A.; Duran, R.; Trillaud, H.; Hocquelet, A. Hepatocellular carcinoma abutting large vessels: Comparison of four percutaneous ablation systems. Int. J. Hyperth. 2018, 34, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Sheiman, R.G.; Mullan, C.; Ahmed, M. In vivo determination of a modified heat capacity of small hepatocellular carcinomas prior to radiofrequency ablation: Correlation with adjacent vasculature and tumour recurrence. Int. J. Hyperth. 2012, 28, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Wakamatsu, T.; Ogasawara, S.; Chiba, T.; Yokoyama, M.; Inoue, M.; Kanogawa, N.; Saito, T.; Suzuki, E.; Ooka, Y.; Tawada, A.; et al. Impact of radiofrequency ablation-induced glisson’s capsule-associated complications in patients with hepatocellular carcinoma. PLoS ONE 2017, 12, e0170153. [Google Scholar] [CrossRef] [PubMed]
- El-Fattah, M.A.; Aboelmagd, M.; Elhamouly, M. Prognostic factors of hepatocellular carcinoma survival after radiofrequency ablation: A US population-based study. United Eur. Gastroenterol. J. 2017, 5, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Kimura, T.; Kita, R.; Osaki, Y. Radiofrequency ablation for hepatocellular carcinoma. Int. J. Hyperth. 2013, 29, 558–568. [Google Scholar] [CrossRef] [PubMed]
- Hirano, G.; Iwata, K.; Anan, A.; Sohda, T.; Kunimoto, H.; Yotsumoto, K.; Fukunaga, A.; Sakurai, K.; Tanaka, T.; Iwashita, H.; et al. Why is radiofrequency ablation therapy applied for hepatocellular carcinoma up to 3 nodules and smaller than 3 cm in tumor size? Hepato-Gastroenterology 2014, 61, 2305–2310. [Google Scholar] [PubMed]
- Na, B.G.; Kim, J.M.; Oh, D.K.; Lee, K.W.; Kang, T.W.; Choi, G.S.; Lee, M.W.; Kwon, C.H.D.; Lim, H.C.; Joh, J.W. Clinical outcomes of laparoscopic radiofrequency ablation of single primary or recurrent hepatocellular carcinoma (≤3 cm). Ann. Surg. Treat. Res. 2017, 92, 355–360. [Google Scholar] [CrossRef] [PubMed]
- European Association For The Study Of The Liver; European Organisation For Research And Treatment Of Cancer. Easl-eortc clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.S.; Raman, S.S.; Vodopich, D.J.; Wang, M.; Sayre, J.; Lassman, C. Effect of vessel size on creation of hepatic radiofrequency lesions in pigs: Assessment of the “heat sink” effect. AJR Am. J. Roentgenol. 2002, 178, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.W.; Zhang, Y.J.; Chen, M.S.; Xu, L.; Liang, H.H.; Lin, X.J.; Guo, R.P.; Zhang, Y.Q.; Lau, W.Y. Radiofrequency ablation with or without transcatheter arterial chemoembolization in the treatment of hepatocellular carcinoma: A prospective randomized trial. J. Clin. Oncol. 2013, 31, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Solbiati, L.; Brace, C.L.; Breen, D.J.; Callstrom, M.R.; Charboneau, J.W.; Chen, M.H.; Choi, B.I.; de Baere, T.; Dodd, G.D., 3rd; et al. Image-guided tumor ablation: Standardization of terminology and reporting criteria—A 10-year update. Radiology 2014, 273, 241–260. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Non-pHV | pHV | p | Non-pPV | pPV | p | Non-Subcapsular | Subcapsular | p |
|---|---|---|---|---|---|---|---|---|---|
| Case Number | 149 | 45 | 156 | 38 | 129 | 65 | |||
| Age (years) | 55.05 ± 12.54 | 57.42 ± 12.61 | 0.269 | 56.04 ± 12.44 | 53.82 ± 13.06 | 0.329 | 54.40 ± 12.33 | 57.98 ± 1.47 | 0.061 |
| Gender (Male/female) | 123/26 | 39/6 | 0.514 | 135/21 | 27/11 | 0.021 * | 108/21 | 54/11 | 0.909 |
| HBV Infection (Y/N) | 123/26 | 40/5 | 0.309 | 130/26 | 33/5 | 0.597 | 109/20 | 54/11 | 0.799 |
| HCV Infection (Y/N) | 8/141 | 1/44 | 0.688 | 8/148 | 1/37 | 1.000 | 6/123 | 3/62 | 1.000 |
| Child-Pugh (A/B) | 147/2 | 42/3 | 0.083 | 152/4 | 37/1 | 1.000 | 124/5 | 65/0 | 0.171 |
| AFP (<400/≥400, ng/mL) | 125/24 | 39/6 | 0.652 | 136/20 | 28/10 | 0.047 * | 111/18 | 53/12 | 0.412 |
| Recurrent HCC (Y/N) | 33/116 | 7/38 | 0.338 | 36/120 | 4/34 | 0.086 | 22/107 | 18/47 | 0.084 |
| Tumor Size (<3/3–5 cm) | 120/29 | 36/9 | 0.937 | 127/29 | 29/9 | 0.478 | 108/21 | 48/17 | 0.102 |
| Cirrhosis (Y/N) | 93/56 | 24/21 | 0.275 | 93/63 | 24/14 | 0.689 | 77/52 | 40/25 | 0.804 |
| Splenomegaly (Y/N) | 54/95 | 18/27 | 0.647 | 58/98 | 14/24 | 0.969 | 48/81 | 24/41 | 0.969 |
| Postoperative Hospital Day | 3.42 ± 2.71 | 3.11 ± 1.32 | 0.468 | 3.40 ± 2.68 | 3.13 ± 1.234 | 0.552 | 3.37 ± 2.84 | 3.29 ± 1.47 | 0.832 |
| RFA Cycle † | 1.43 ± 0.60 | 1.53 ± 0.66 | 0.352 | 1.41 ± 0.58 | 1.65 ± 0.71 | 0.025 * | 1.43 ± 0.60 | 1.52 ± 0.64 | 0.300 |
| Operation Failure †† | 8/142 | 3/42 | 0.718 | 6/151 | 5/33 | 0.041 * | 8/122 | 3/62 | 0.755 |
| Factor | OS | RFS | rRFS | dRFS | ||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Older age (≥55 vs. <55, years) | 1.94 (1.07–3.52) | 0.030 * | 0.87 (0.61–1.26) | 0.468 | 0.79 (0.48–1.32) | 0.372 | 1.02 (0.68–1.51) | 0.938 |
| Cirrhosis | 2.26 (1.18–4.34) | 0.014 * | 1.14 (0.79–1.65) | 0.488 | 1.13 (0.67–1.90) | 0.654 | 1.13 (0.75–1.69) | 0.567 |
| Splenomegaly | 2.15 (1.23–3.78) | 0.008 * | 0.97 (0.66–1.42) | 0.886 | 0.93 (0.54–1.59) | 0.780 | 1.06 (0.70–1.60) | 0.798 |
| Peri-hepatic-vein location | 1.55 (0.83–2.89) | 0.174 | 1.18 (0.77–1.80) | 0.455 | 1.98 (1.15–3.40) | 0.013 * | 0.95 (0.59–1.55) | 0.849 |
| ALT level (≥35 vs. <35, U/L) | 1.08 (0.60–1.93) | 0.795 | 1.38 (0.96–2.00) | 0.083 | 0.96 (0.56–1.64) | 0.868 | 1.67 (1.12–2.49) | 0.012 * |
| AFP level (≥400 vs. <400, ng/mL) | 1.13 (0.53–2.40) | 0.761 | 1.58 (1.00–2.49) | 0.049 * | 1.00 (0.49–2.03) | 0.999 | 1.53 (0.92–2.52) | 0.098 |
| Child–Pugh score | 3.47 (2.27–5.31) | <0.001 * | 1.04 (0.66–1.64) | 0.881 | 1.39 (0.83–2.33) | 0.212 | 1.15 (0.71–1.86) | 0.569 |
| Size level (3–5 vs. <3, cm) | 1.38 (0.73–2.60) | 0.32 | 1.00 (0.63–1.57) | 0.992 | 1.36 (0.74–2.47) | 0.32 | 0.89 (0.53–1.49) | 0.662 |
| Recurrent tumor | 0.77 (0.36–1.65) | 0.503 | 1.38 (0.91–2.10) | 0.127 | 0.93 (0.50–1.76) | 0.834 | 1.31 (0.83–2.06) | 0.248 |
| Factor | HR (95% CI) | p Value |
|---|---|---|
| Older age (≥55 vs. <55, years) | 2.00 (1.08–3.69) | 0.028 * |
| Cirrhosis | 1.82 (0.88–3.74) | 0.105 |
| Splenomegaly | 1.49 (0.77–2.85) | 0.233 |
| Child–Pugh score | 2.67 (1.70–4.19) | <0.001 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.; Peng, K.; Hu, D.; Shen, J.; Zhou, Z.; Xu, L.; Chen, J.; Pan, Y.; Wang, J.; Zhang, Y.; et al. Tumor Location Influences Oncologic Outcomes of Hepatocellular Carcinoma Patients Undergoing Radiofrequency Ablation. Cancers 2018, 10, 378. https://doi.org/10.3390/cancers10100378
Chen J, Peng K, Hu D, Shen J, Zhou Z, Xu L, Chen J, Pan Y, Wang J, Zhang Y, et al. Tumor Location Influences Oncologic Outcomes of Hepatocellular Carcinoma Patients Undergoing Radiofrequency Ablation. Cancers. 2018; 10(10):378. https://doi.org/10.3390/cancers10100378
Chicago/Turabian StyleChen, Jinbin, Kangqiang Peng, Dandan Hu, Jingxian Shen, Zhongguo Zhou, Li Xu, Jiancong Chen, Yangxun Pan, Juncheng Wang, Yaojun Zhang, and et al. 2018. "Tumor Location Influences Oncologic Outcomes of Hepatocellular Carcinoma Patients Undergoing Radiofrequency Ablation" Cancers 10, no. 10: 378. https://doi.org/10.3390/cancers10100378