Closing the Gender Gap in Fragile X Syndrome: Review of Females with Fragile X Syndrome and Preliminary Research Findings

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction to Fragile X Syndrome
2. Genetics
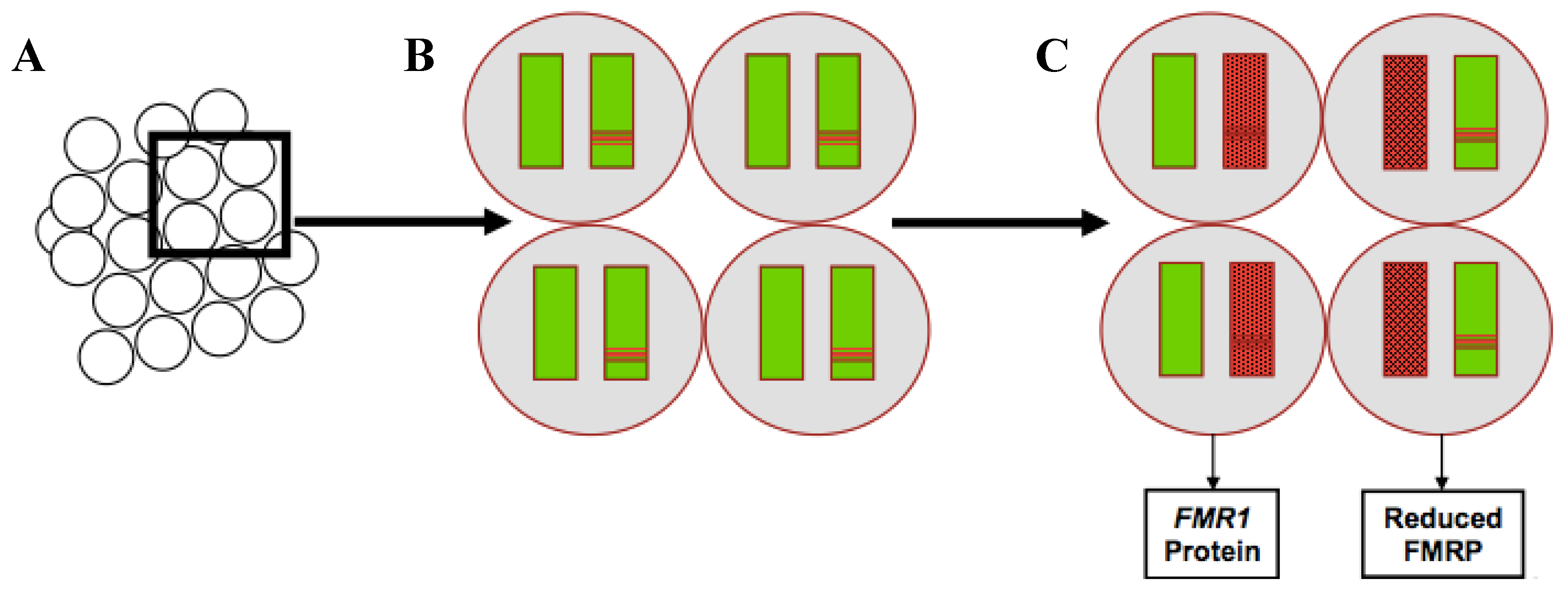
2.1. Pattern of Inheritance of Fragile X Syndrome
2.2. Genetic Foundation of Sex Differences
3. The Fragile X Phenotype in Females
3.1. Cognitive Effects
3.2. Socio-Emotional Effects
3.3. Adaptive Behavior and Independent Living
3.4. Barriers to Positive Outcomes
4. Methods
4.1. Participants
4.2. Measurements/Procedures
4.2.1. Cognition and Academics
4.2.2. Child Behavior and Emotion
4.2.3. Adaptive Behavior and Functional Skills
4.3. Data Analyses
4.4. Preliminary Findings
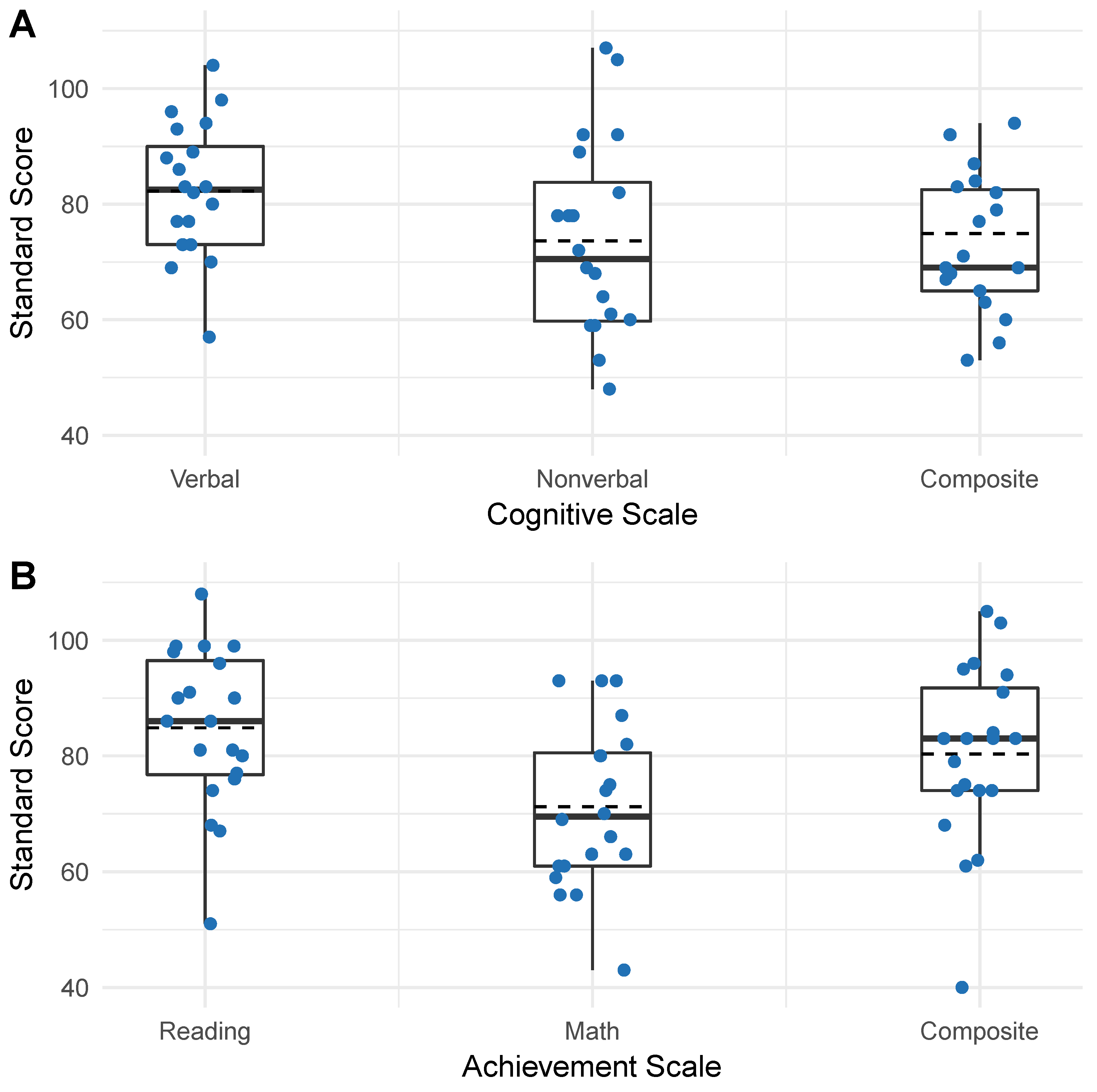
4.4.1. Cognition and Academics
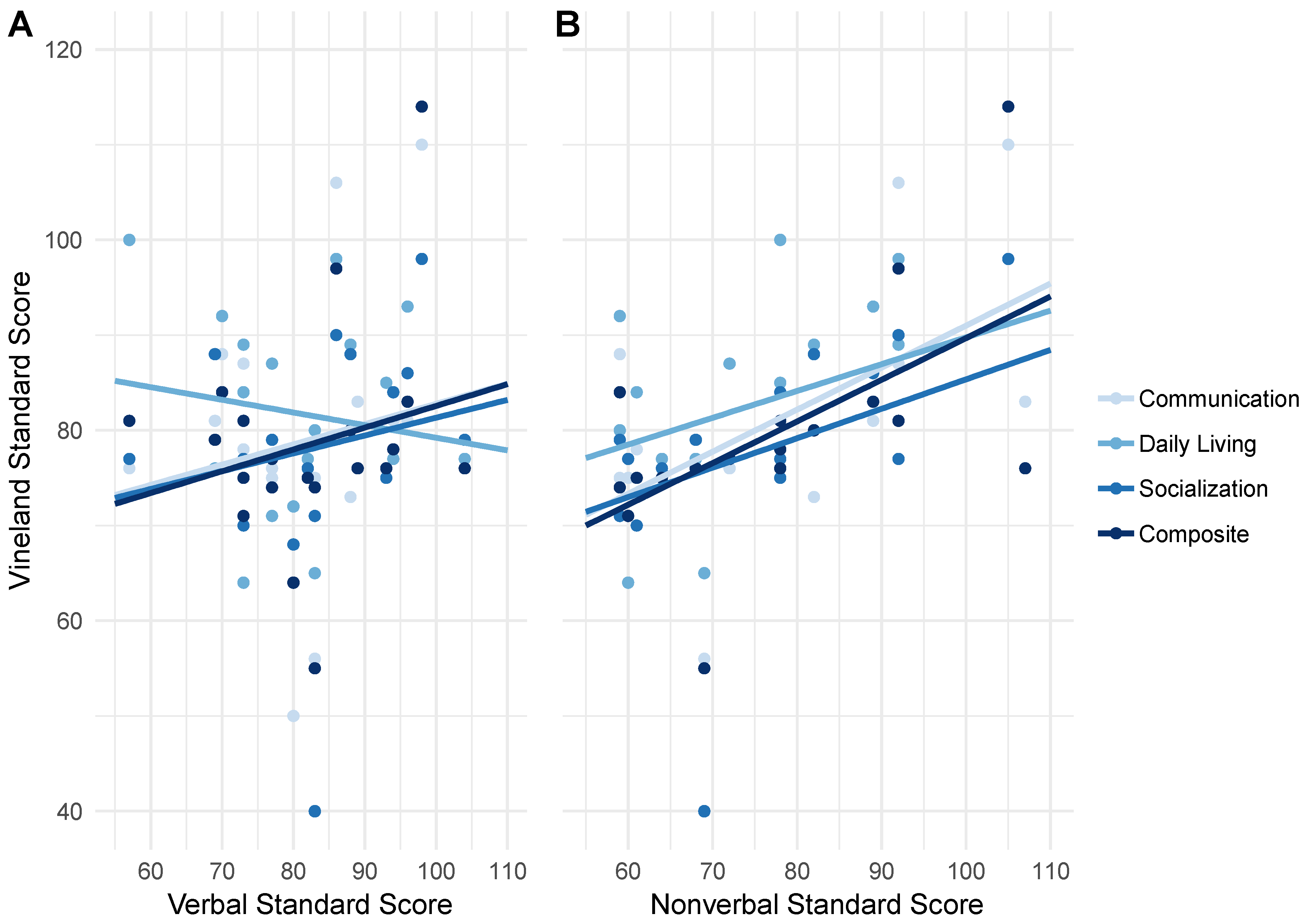
4.4.2. Correlations between Cognition and Adaptive Behavior
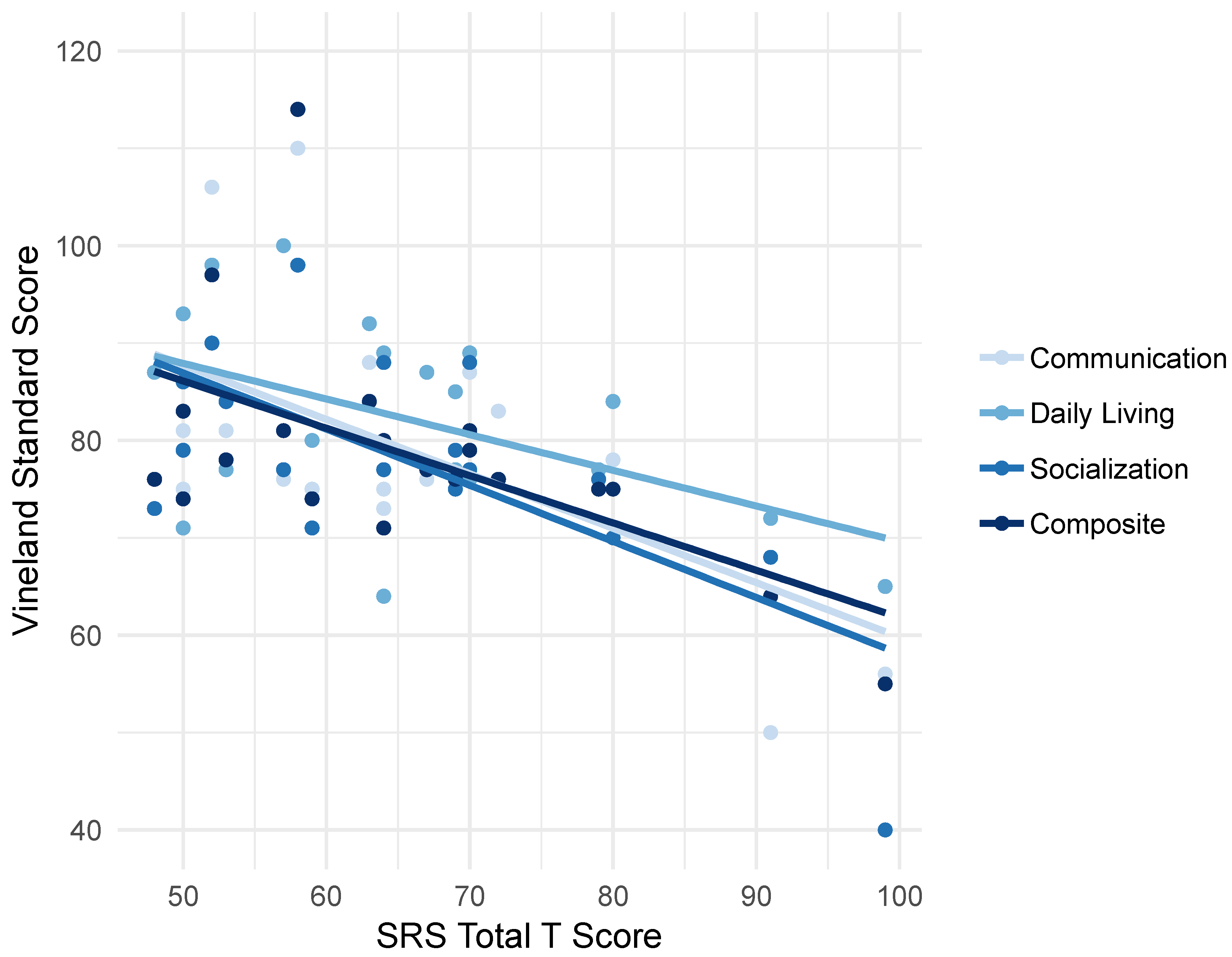
4.4.3. Correlations between Social Skills and Adaptive Behavior
5. Discussion
5.1. Cognition and Academics
5.2. Adaptive Behavior Outcomes
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hunter, J.; Rivero-Arias, O.; Angelov, A.; Kim, E.; Fotheringham, I.; Leal, J. Epidemiology of fragile X syndrome: A systematic review and meta-analysis. Am. J. Med. Genet. Part A 2014. [Google Scholar] [CrossRef] [PubMed]
- Hagerman, P.J. The fragile X prevalence paradox. J. Med. Genet. 2008, 5, 498–499. [Google Scholar] [CrossRef] [PubMed]
- Crawford, D.C.; Acuña, J.M.; Sherman, S.L. FMR1 and the fragile X syndrome: Human genome epidemiology review. Genet. Med. 2001, 3, 359–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, D.B.; Raspa, M.; Olmsted, M.; Holiday, D.B. Co-occurring conditions associated with FMR1 gene variations: Findings from a national parent survey. Am. J. Med. Genet. Part A 2008, 146, 2060–2069. [Google Scholar] [CrossRef] [PubMed]
- Hagerman, R.J.; Berry-Kravis, E.; Hazlett, H.C.; Bailey, D.B.; Moine, H.; Kooy, R.F.; Tassone, F.; Gantois, I.; Sonenberg, N.; Mandel, J.L.; et al. Fragile X syndrome. Nat. Rev. Dis. Prim. 2017, 3, 17065. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, A.; Hallahan, B. Fragile X-associated disorders: A clinical overview. J. Neurol. 2012, 259, 401–413. [Google Scholar] [CrossRef]
- Bambang, K.; Metcalfe, K.; Newman, W.; McFarlane, T. Fragile X syndrome: An overview. Obstet. Gynaecol. 2011, 13, 92–97. [Google Scholar] [CrossRef]
- Garber, K.B.; Visootsak, J.; Warren, S.T. Fragile X syndrome. Eur. J. Hum. Genet. 2008. [Google Scholar] [CrossRef]
- Bagni, C.; Oostra, B.A. Fragile X syndrome: From protein function to therapy. Am. J. Med. Genet. Part A 2013, 161, 2809–2821. [Google Scholar] [CrossRef]
- Reiss, A.L.; Hall, S.S. Fragile X Syndrome: Assessment and Treatment Implications. Child Adolesc. Psychiatr. Clin. N. Am. 2007, 16, 663–675. [Google Scholar] [CrossRef]
- Loesch, D.Z.; Huggins, R.M.; Hagerman, R.J. Phenotypic Variation and FMRP Levels in Fragile X. Ment. Retard. Dev. Disabil. Res. Rev. 2004, 10, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Tassone, F.; Hagerman, R.J.; Iklé, D.N.; Dyer, P.N.; Lampe, M.; Willemsen, R.; Oostra, B.A.; Taylor, A.K. FMRP expression as a potential prognostic indicator in fragile X syndrome. Am. J. Med. Genet. 1999. [Google Scholar] [CrossRef]
- Del Hoyo Soriano, L.; Thurman, A.J.; Harvey, D.J.; Ted Brown, W.; Abbeduto, L. Genetic and maternal predictors of cognitive and behavioral trajectories in females with fragile X syndrome. J. Neurodev. Disord. 2018. [Google Scholar] [CrossRef] [PubMed]
- Di, K.N.; Disteche, C.M. Dosage compensation of the active X chromosome in mammals. Nat. Genet. 2006. [Google Scholar] [CrossRef]
- Glaser, B.; Hessl, D.; Dyer-Friedman, J.; Johnston, C.; Wisbeck, J.; Taylor, A.; Reiss, A. Biological and environmental contributions to adaptive behavior in fragile X syndrome. Am. J. Med. Genet. 2003. [Google Scholar] [CrossRef] [PubMed]
- Reiss, A.L.; Dant, C.C. The behavioral neurogenetics of fragile X syndrome: Analyzing gene-brain-behavior relationships in child developmental psychopathologies. Dev. Psychopathol. 2003. [Google Scholar] [CrossRef]
- Hartley, S.L.; Seltzer, M.M.; Raspa, M.; Olmstead, M.; Bishop, E.; Bailey, D.B. Exploring the adult life of men and women with fragile X syndrome: Results from a national survey. Am. J. Intellect. Dev. Disabil. 2011, 116, 16–35. [Google Scholar] [CrossRef]
- Hagerman, R.J.; Jackson, C.; Amiri, K.; Silverman, A.C.; O’Connor, R.; Sobesky, W. Girls with fragile X syndrome: Physical and neurocognitive status and outcome. Pediatrics 1992, 89, 395–400. [Google Scholar]
- Kogan, C.S.; Boutet, I.; Cornish, K.; Graham, G.E.; Berry-Kravis, E.; Drouin, A.; Milgram, N.W. A comparative neuropsychological test battery differentiates cognitive signatures of Fragile X and Down syndrome. J. Intell. Disabil. Res. 2009. [Google Scholar] [CrossRef]
- Bennetto, L.; Pennington, B.F.; Porter, D.; Taylor, A.K.; Hagerman, R.J. Profile of cognitive functioning in women with the fragile X mutation. Neuropsychology 2001. [Google Scholar] [CrossRef]
- Freund, L.S.; Reiss, A.L.; Abrams, M.T. Psychiatric disorders associated with fragile X in the young female. Pediatrics 1993, 91, 321–329. [Google Scholar] [PubMed]
- Schwarte, A.R. Fragile X Syndrome. Sch. Psychol. Q. 2008. [Google Scholar] [CrossRef]
- Cornish, K. Cognitive strengths and difficulties. In Educating Children with Fragile X: A Multi-Professional Handbook; Dew-Hughes, D., Ed.; RoutledgeFalmer: London, UK, 2004; pp. 20–24. ISBN 0203561538. [Google Scholar]
- Lightbody, A.A.; Hall, S.S.; Reiss, A.L. Chronological age, but not FMRP levels, predicts neuropsychological performance in girls with fragile X syndrome. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2006. [Google Scholar] [CrossRef] [PubMed]
- NIMH National Institute of Mental Health Research Domain Criteria (RDoC) Constucts. Available online: https://www.nimh.nih.gov/research-priorities/rdoc/constructs/negative-valence-systems.shtml (accessed on 30 November 2018).
- Cordeiro, L.; Ballinger, E.; Hagerman, R.; Hessl, D. Clinical assessment of DSM-IV anxiety disorders in fragile X syndrome: Prevalence and characterization. J. Neurodev. Disord. 2011, 3, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Hessl, D.; Glaser, B.; Dyer-Friedman, J.; Reiss, A.L. Social behavior and cortisol reactivity in children with fragile X syndrome. J. Child Psychol. Psychiatry Allied Discip. 2006, 47, 602–610. [Google Scholar] [CrossRef]
- Hall, S.S.; Lightbody, A.A.; Huffman, L.C.; Lazzeroni, L.C.; Reiss, A.L. Physiological correlates of social avoidance behavior in children and adolescents with fragile x syndrome. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Mazzocco, M.M.M.; Kates, W.R.; Baumgardner, T.L.; Freund, L.S.; Reiss, A.L. Autistic behaviors among girls with fragile X syndrome. J. Autism Dev. Disord. 1997, 27, 415–435. [Google Scholar] [CrossRef]
- Lesniak-Karpiak, K.; Mazzocco, M.M.M.; Ross, J.L. Behavioral assessment of social anxiety in females with turner or fragile X syndrome. J. Autism Dev. Disord. 2003. [Google Scholar] [CrossRef]
- Hatton, D.D.; Wheeler, A.C.; Skinner, M.L.; Bailey, D.B.; Sullivan, K.M.; Roberts, J.E.; Mirrett, P.; Clark, R.D. Adaptive behavior in children with fragile X syndrome. Am. J. Ment. Retard. 2003. [Google Scholar] [CrossRef]
- Klaiman, C.; Quintin, E.-M.; Jo, B.; Lightbody, A.A.; Hazlett, H.C.; Piven, J.; Hall, S.S.; Chromik, L.C.; Reiss, A.L. Longitudinal profiles of adaptive behavior in fragile X syndrome. Pediatrics 2014, 134, 315–324. [Google Scholar] [CrossRef]
- Bailey, D.B.; Raspa, M.; Holiday, D.; Bishop, E.; Olmsted, M. Functional skills of individuals with fragile X syndrome: A lifespan cross-sectional analysis. Am. J. Intellect. Dev. Disabil. 2009. [Google Scholar] [CrossRef] [PubMed]
- Hustyi, K.M.; Hall, S.S.; Quintin, E.M.; Chromik, L.C.; Lightbody, A.A.; Reiss, A.L. The Relationship Between Autistic Symptomatology and Independent Living Skills in Adolescents and Young Adults with Fragile X Syndrome. J. Autism Dev. Disord. 2015, 45, 1836–1844. [Google Scholar] [CrossRef] [PubMed]
- Hessl, D.; Dyer-Friedman, J.; Glaser, B.; Wisbeck, J.; Barajas, R.G.; Taylor, A.; Reiss, A.L. The Influence of Environmental and Genetic Factors on Behavior Problems and Autistic Symptoms in Boys and Girls with Fragile X Syndrome. Pediatrics 2001. [Google Scholar] [CrossRef]
- Dyer-Friedman, J.; Glaser, B.; Hessl, D.; Johnston, C.; Huffman, L.C.; Taylor, A.; Wisbeck, J.; Reiss, A.L. Genetic and Environmental Influences on the Cognitive Outcomes of Children with Fragile X Syndrome. J. Am. Acad. Child Adolesc. Psychiatry 2002. [Google Scholar] [CrossRef]
- Elliott, C.D. Differential Ability Scales, 2nd ed.; NCS Pearson, Inc.: Minneapolis, MN, USA, 2007. [Google Scholar]
- Kaufman, A.S.; Kaufman, N.L. Kaufman Test of Educational Achievement, Third Edition Brief Form (KTEA-3 Brief); NCS Pearson, Inc.: Minneapolis, MN, USA, 2015. [Google Scholar]
- Constantino, J.N.; Gruber, C.P. Social Responsiveness Scale (SRS), 2nd ed.; Western Psychological Services: Los Angeles, CA, USA, 2012. [Google Scholar]
- Sparrow, S.S.; Cicchetti, D.V.; Balla, D.A. Vineland-II Adaptive Behavior Scales: Survey Forms Manual; NCS Pearson, Inc.: Minneapolis, MN, USA, 2005. [Google Scholar]
- Freund, L.S.; Reiss, A.L. Cognitive profiles associated with the fra(X) syndrome in males and females. Am. J. Med. Genet. 1991, 38, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Braden, M. The effect of fragile X syndrome on learning. In Educating Children with Fragile X: A Multi-Professional Handbook; Dew-Hughes, D., Ed.; RoutledgeFalmer: London, UK, 2003; pp. 43–47. ISBN 0203561538. [Google Scholar]
- Kemper, M.B.; Hagerman, R.J.; Altshul-Stark, D. Cognitive profiles of boys with the fragile X syndrome. Am. J. Med. Genet. 1988, 30, 191–200. [Google Scholar] [CrossRef] [PubMed]





© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartholomay, K.L.; Lee, C.H.; Bruno, J.L.; Lightbody, A.A.; Reiss, A.L. Closing the Gender Gap in Fragile X Syndrome: Review of Females with Fragile X Syndrome and Preliminary Research Findings. Brain Sci. 2019, 9, 11. https://doi.org/10.3390/brainsci9010011
Bartholomay KL, Lee CH, Bruno JL, Lightbody AA, Reiss AL. Closing the Gender Gap in Fragile X Syndrome: Review of Females with Fragile X Syndrome and Preliminary Research Findings. Brain Sciences. 2019; 9(1):11. https://doi.org/10.3390/brainsci9010011
Chicago/Turabian StyleBartholomay, Kristi L., Cindy H. Lee, Jennifer L. Bruno, Amy A. Lightbody, and Allan L. Reiss. 2019. "Closing the Gender Gap in Fragile X Syndrome: Review of Females with Fragile X Syndrome and Preliminary Research Findings" Brain Sciences 9, no. 1: 11. https://doi.org/10.3390/brainsci9010011