Location-Dependent Patient Outcome and Recurrence Patterns in IDH1-Wildtype Glioblastoma

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Location-Dependent IDH1 Mutation Status and Treatment-Inherent Differences
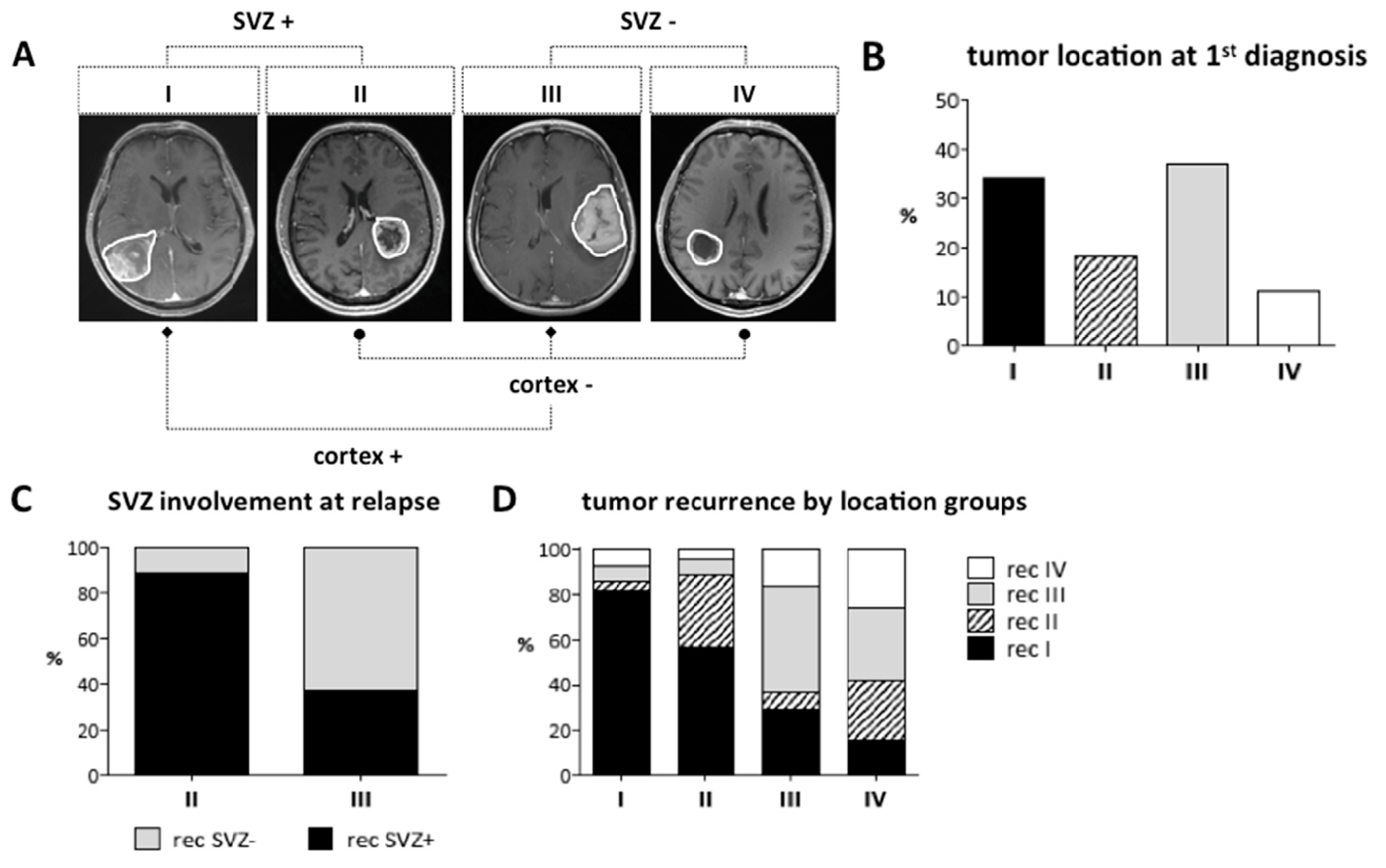
2.2. Location-Dependent Growth and Recurrence
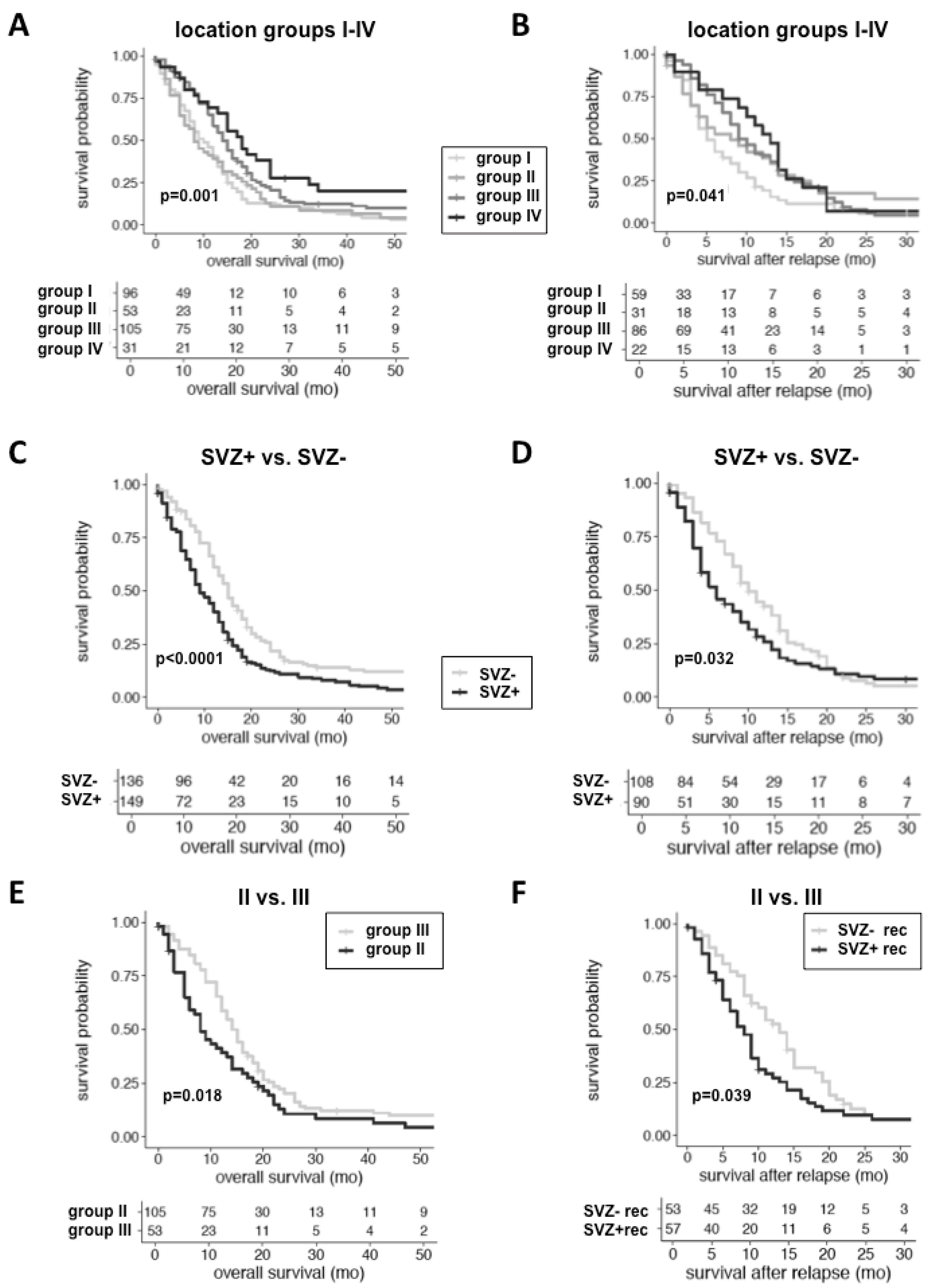
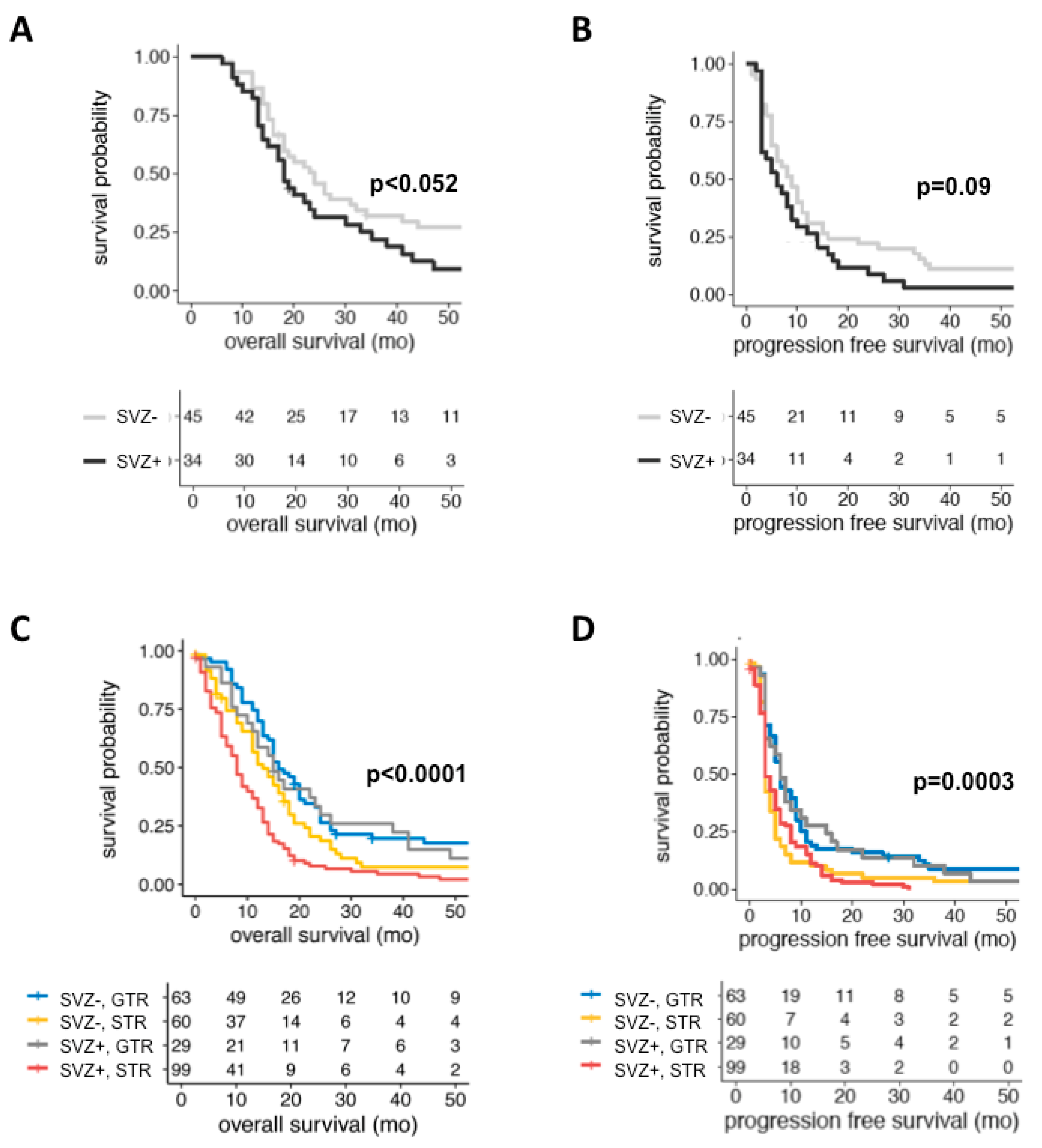
2.3. Location-Dependent Patient Outcome
3. Discussion
4. Materials and Methods
4.1. Patient Cohort
4.2. Radiographic Analysis
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| GBM | glioblastoma |
| WHO | World Health Organization |
| TMZ | temozolomide |
| LTS | long-term survivor |
| NSC | neural stem cell |
| NPC | neural progenitor cell |
| SVZ | subventricular zone |
| PFS | progression-free survival |
| OS | overall survival |
| IDH1 | isocitrate dehydrogenase 1 |
| CEL | contrast-enhancing lesion |
| KPS | Karnofsky performance score |
| GTR | gross total resection |
| EOR | extent of resection |
| STS | short-term survivor |
| MGMT | O6-methylguanin-DNA-methyltransferase |
| CE | contrast-enhancing |
| T1-w | T1-weighted |
| FLAIR | fluid-attenuated inversion recovery |
| RT | radiotherapy |
| HR | hazard ratio |
| CI | confidence intervall |
| PACS | Picture Archiving and Communication System |
| RANO | Response Assessment in Neuro-Oncology |
| MPRAGE | magnetization-prepared rapid gradient-echo |
References
- Stupp, R.; Mason, W.P.; Van Den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Krex, D.; Klink, B.; Hartmann, C.; von Deimling, A.; Pietsch, T.; Simon, M.; Sabel, M.; Steinbach, J.P.; Heese, O.; Reifenberger, G.; et al. Long-term survival with glioblastoma multiforme. Brain J. Neurol. 2007, 130, 2596–2606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanai, N.; Tramontin, A.D.; Quinones-Hinojosa, A.; Barbaro, N.M.; Gupta, N.; Kunwar, S.; Lawton, M.T.; McDermott, M.W.; Parsa, A.T.; Verdugo, J.M.; et al. Unique astrocyte ribbon in adult human brain contains neural stem cells but lacks chain migration. Nature 2004, 427, 740–744. [Google Scholar] [CrossRef] [PubMed]
- Sanai, N.; Alvarez-Buylla, A.; Berger, M.S. Neural stem cells and the origin of gliomas. N. Engl. J. Med. 2005, 353, 811–822. [Google Scholar] [CrossRef] [PubMed]
- Llaguno, S.A.; Chen, J.; Kwon, C.H.; Jackson, E.L.; Li, Y.; Burns, D.K.; Alvarez-Buylla, A.; Parada, L.F. Malignant astrocytomas originate from neural stem/progenitor cells in a somatic tumor suppressor mouse model. Cancer Cell 2009, 15, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Kwon, C.H.; Zhao, D.; Chen, J.; Alcantara, S.; Li, Y.; Burns, D.K.; Mason, R.P.; Eva, Y.H.; Wu, H.; Parada, L.F. Pten haploinsufficiency accelerates formation of high-grade astrocytomas. Cancer Res. 2008, 68, 3286–3294. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Guignard, F.; Zhao, D.; Liu, L.; Burns, D.K.; Mason, R.P.; Messing, A.; Parada, L.F. Early inactivation of p53 tumor suppressor gene cooperating with NF1 loss induces malignant astrocytoma. Cancer Cell 2005, 8, 119–130. [Google Scholar] [CrossRef] [Green Version]
- Holland, E.C.; Celestino, J.; Dai, C.; Schaefer, L.; Sawaya, R.E.; Fuller, G.N. Combined activation of Ras and Akt in neural progenitors induces glioblastoma formation in mice. Nat. Genet. 2000, 25, 55–57. [Google Scholar] [CrossRef]
- Piccirillo, S.G.; Dietz, S.; Madhu, B.; Griffiths, J.; Price, S.J.; Collins, V.P.; Watts, C. Fluorescence-guided surgical sampling of glioblastoma identifies phenotypically distinct tumour-initiating cell populations in the tumour mass and margin. Br. J. Cancer 2012, 107, 462–468. [Google Scholar] [CrossRef] [Green Version]
- Gupta, T.; Nair, V.; Jalali, R. Stem cell niche irradiation in glioblastoma: Providing a ray of hope? CNS Oncol. 2014, 3, 367–376. [Google Scholar] [CrossRef]
- Chaichana, K.L.; McGirt, M.J.; Frazier, J.; Attenello, F.; Guerrero-Cazares, H.; Quinones-Hinojosa, A. Relationship of glioblastoma multiforme to the lateral ventricles predicts survival following tumor resection. J. Neurooncol. 2008, 89, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Kappadakunnel, M.; Eskin, A.; Dong, J.; Nelson, S.F.; Mischel, P.S.; Liau, L.M.; Ngheimphu, P.; Lai, A.; Cloughesy, T.F.; Goldin, J.; et al. Stem cell associated gene expression in glioblastoma multiforme: Relationship to survival and the subventricular zone. J. Neurooncol. 2010, 96, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Jafri, N.F.; Clarke, J.L.; Weinberg, V.; Barani, I.J.; Cha, S. Relationship of glioblastoma multiforme to the subventricular zone is associated with survival. Neuro-Oncol. 2013, 15, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Young, G.S.; Macklin, E.A.; Setayesh, K.; Lawson, J.D.; Wen, P.Y.; Norden, A.D.; Drappatz, J.; Kesari, S. Longitudinal MRI evidence for decreased survival among periventricular glioblastoma. J. Neurooncol. 2011, 104, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Adeberg, S.; Bostel, T.; König, L.; Welzel, T.; Debus, J.; Combs, S.E. A comparison of long-term survivors and short-term survivors with glioblastoma, subventricular zone involvement: A predictive factor for survival? Radiat. Oncol. Lond. Engl. 2014, 9, 95. [Google Scholar] [CrossRef] [PubMed]
- Mistry, A.M.; Hale, A.T.; Chambless, L.B.; Weaver, K.D.; Thompson, R.C.; Ihrie, R.A. Influence of glioblastoma contact with the lateral ventricle on survival: A meta-analysis. J. Neurooncol. 2017, 131, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Noushmehr, H.; Weisenberger, D.J.; Diefes, K.; Phillips, H.S.; Pujara, K.; Berman, B.P.; Pan, F.; Pelloski, C.E.; Sulman, E.P.; Bhat, K.P.; et al. Identification of a CpG island methylator phenotype that defines a distinct subgroup of glioma. Cancer Cell 2010, 17, 510–522. [Google Scholar] [CrossRef]
- Turcan, S.; Rohle, D.; Goenka, A.; Walsh, L.A.; Fang, F.; Yilmaz, E.; Campos, C.; Fabius, A.W.; Lu, C.; Ward, P.S.; et al. IDH1 mutation is sufficient to establish the glioma hypermethylator phenotype. Nature 2012, 483, 479–483. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef]
- Lim, D.A.; Cha, S.; Mayo, M.C.; Chen, M.H.; Keles, E.; VandenBerg, S.; Berger, M.S. Relationship of glioblastoma multiforme to neural stem cell regions predicts invasive and multifocal tumor phenotype. Neuro-Oncol. 2007, 9, 424–429. [Google Scholar] [CrossRef] [Green Version]
- Adeberg, S.; König, L.; Bostel, T.; Harrabi, S.; Welzel, T.; Debus, J.; Combs, S.E. Glioblastoma recurrence patterns after radiation therapy with regard to the subventricular zone. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Lee, Y.; Miller, R.; Castillo, M. Glioblastoma multiforme: Relationship to subventricular zone and recurrence. Neuroradiol. J. 2013, 26, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Bohman, L.E.; Swanson, K.R.; Moore, J.L.; Rockne, R.; Mandigo, C.; Hankinson, T.; Assanah, M.; Canoll, P.; Bruce, J.N. Magnetic resonance imaging characteristics of glioblastoma multiforme: Implications for understanding glioma ontogeny. Neurosurgery 2010, 67, 1319–1327. [Google Scholar] [CrossRef] [PubMed]
- Batista, K.M.; Vega, I.F.; de Eulate-Beramendi, S.A.; Morales, J.C.; Kurbanov, A.; Asnel, D.; Meilan, A.; Astudillo, A. Prognostic significance of the markers IDH1 and YKL40 related to the subventricular zone. Folia Neuropathol. 2015, 53, 52–59. [Google Scholar] [CrossRef]
- Patil, C.G.; Yi, A.; Elramsisy, A.; Hu, J.; Mukherjee, D.; Irvin, D.K.; John, S.Y.; Bannykh, S.I.; Black, K.L.; Nuño, M. Prognosis of patients with multifocal glioblastoma: A case-control study. J. Neurosurg. 2012, 117, 705–711. [Google Scholar] [CrossRef]
- Thomas, R.P.; Xu, L.W.; Lober, R.M.; Li, G.; Nagpal, S. The incidence and significance of multiple lesions in glioblastoma. J. Neurooncol. 2013, 112, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Lasocki, A.; Gaillard, F.; Tacey, M.; Drummond, K.; Stuckey, S. Multifocal and multicentric glioblastoma: Improved characterisation with FLAIR imaging and prognostic implications. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2016, 31, 92–98. [Google Scholar] [CrossRef]
- Lee, J.K.; Wang, J.; Sa, J.K.; Ladewig, E.; Lee, H.O.; Lee, I.H.; Kang, H.J.; Rosenbloom, D.S.; Camara, P.G.; Liu, Z.; et al. Spatiotemporal genomic architecture informs precision oncology in glioblastoma. Nat. Genet. 2017, 49, 594–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abou-El-Ardat, K.; Seifert, M.; Becker, K.; Eisenreich, S.; Lehmann, M.; Hackmann, K.; Rump, A.; Meijer, G.; Carvalho, B.; Temme, A.; et al. Comprehensive molecular characterization of multifocal glioblastoma proves its monoclonal origin and reveals novel insights into clonal evolution and heterogeneity of glioblastomas. Neuro-Oncol. 2017, 19, 546–557. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, M.C. Radiographic patterns of relapse in glioblastoma. J. Neurooncol. 2011, 101, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Petrecca, K.; Guiot, M.-C.; Panet-Raymond, V.; Souhami, L. Failure pattern following complete resection plus radiotherapy and temozolomide is at the resection margin in patients with glioblastoma. J. Neurooncol. 2013, 111, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Brandes, A.A.; Tosoni, A.; Franceschi, E.; Sotti, G.; Frezza, G.; Amista, P.; Morandi, L.; Spagnolli, F.; Ermani, M. Recurrence pattern after temozolomide concomitant with and adjuvant to radiotherapy in newly diagnosed patients with glioblastoma: Correlation with MGMT promoter methylation status. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 1275–1279. [Google Scholar] [CrossRef]
- De Bonis, P.; Anile, C.; Pompucci, A.; Fiorentino, A.; Balducci, M.; Chiesa, S.; Lauriola, L.; Maira, G.; Mangiola, A. The influence of surgery on recurrence pattern of glioblastoma. Clin. Neurol. Neurosurg. 2013, 115, 37–43. [Google Scholar] [CrossRef]
- Tejada, S.; Díez-Valle, R.; Aldave, G.; Marigil, M.; de Gallego, J.; Domínguez, P.D. Factors associated with a higher rate of distant failure after primary treatment for glioblastoma. J. Neurooncol. 2014, 116, 169–175. [Google Scholar] [CrossRef]
- Kim, J.; Lee, I.H.; Cho, H.J.; Park, C.K.; Jung, Y.S.; Kim, Y.; Nam, S.H.; Kim, B.S.; Johnson, M.D.; Kong, D.S.; et al. Spatiotemporal Evolution of the Primary Glioblastoma Genome. Cancer Cell 2015, 28, 318–328. [Google Scholar] [CrossRef] [Green Version]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.M.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients with Glioblastoma: A Randomized Clinical Trial. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef]
- Jungk, C.; Mock, A.; Exner, J.; Geisenberger, C.; Warta, R.; Capper, D.; Abdollahi, A.; Friauf, S.; Lahrmann, B.; Grabe, N.; et al. Spatial transcriptome analysis reveals Notch pathway-associated prognostic markers in IDH1 wild-type glioblastoma involving the subventricular zone. BMC Med. 2016, 14, 170. [Google Scholar] [CrossRef] [PubMed]
- Capper, D.; Weißert, S.; Balss, J.; Habel, A.; Meyer, J.; Jäger, D.; Ackermann, U.; Tessmer, C.; Korshunov, A.; Zentgraf, H.; et al. Characterization of R132H mutation-specific IDH1 antibody binding in brain tumors. Brain Pathol. 2010, 20, 245–254. [Google Scholar] [CrossRef]
- Hartmann, C.; Meyer, J.; Balss, J.; Capper, D.; Mueller, W.; Christians, A.; Felsberg, J.; Wolter, M.; Mawrin, C.; Wick, W.; et al. Type and frequency of IDH1 and IDH2 mutations are related to astrocytic and oligodendroglial differentiation and age: A study of 1,010 diffuse gliomas. Acta Neuropathol. 2009, 118, 469–474. [Google Scholar] [CrossRef]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; DeGroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated response assessment criteria for high-grade gliomas: Response assessment in neuro-oncology working group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients; n (%) | Group I | Group II | Group III | Group IV | Total | All | SVZ +/− | cortex +/− | II vs. III |
|---|---|---|---|---|---|---|---|---|---|
| 96 (34) | 53 (18) | 105 (37) | 31 (11) | 285 (100) | p-value | ||||
| Age (years); median (range) | 67 (20–84) | 60 (30–81) | 61 (36–87) | 64 (38–78) | 64 (20–87) | 0.095 | 0.404 | 0.218 | 0.443 |
| Sex; n (male/female) | 58/38 | 34/19 | 67/38 | 19/12 | 178/107 | 0.953 | 0.808 | 1.0 | 1.0 |
| KPS pre-op; median (range) | 85 (20–100) | 80 (30–100) | 90 (40–100) | 90 (50–100) | 90 (20–100) | 0.002 | <0.001 | 0.092 | 0.002 |
| Survival Data | |||||||||
| Death; n (%) | 93 (97) | 49 (91) | 95 (90) | 25 (81) | 272 (95) | 0.032 | 0.031 | 0.152 | 0.775 |
| OS (months); median (range) | 10 (0–69) | 8 (0–83) | 14 (0–99) | 18 (0–68) | 12 (0–99) | <0.001 | <0.0001 | 0.701 | 0.018 |
| PFS (months); median (range) | 4.5 (0–57) | 3 (0–43) | 4 (0–90) | 5 (0–57) | 4 (0–90) | 0.197 | 0.189 | 0.978 | 0.271 |
| Survival after relapse (months); median (range) | 5 (0–49) | 6 (0–43) | 9 (0–78) | 11.5 (0–63) | 8 (0–78) | 0.041 | 0.032 | 0.286 | 0.91 |
| LTS (> 36 months); n (%) | 7 (7) | 4 (8) | 11 (10) | 5 (16) | 27 (9) | 0.478 | 0.229 | 0.66 | 0.775 |
| STS (> 6 < 10 months); n (%) | 21 (22) | 11 (20) | 16 (15) | 4 (13) | 52 (18) | 0.512 | 0.167 | 1.0 | 0.381 |
| Molecular Data (n = 285) | |||||||||
| MGMT meth; n (%) - Yes - No - N/A | 96 (100) 32 (33) 24 (25) 40 (42) | 53 (100) 14 (26) 16 (31) 23 (43) | 105 (100) 20 (19) 42 (40) 43 (41) | 31 (100) 9 (29) 12 (39) 10 (32) | 285 (100) 75 (26) 94 (33) 116 (41) | 0.203 | 0.045 | 0.944 | 0.394 |
| Radiographic Characteristics at 1st Diagnosis (n = 285) | |||||||||
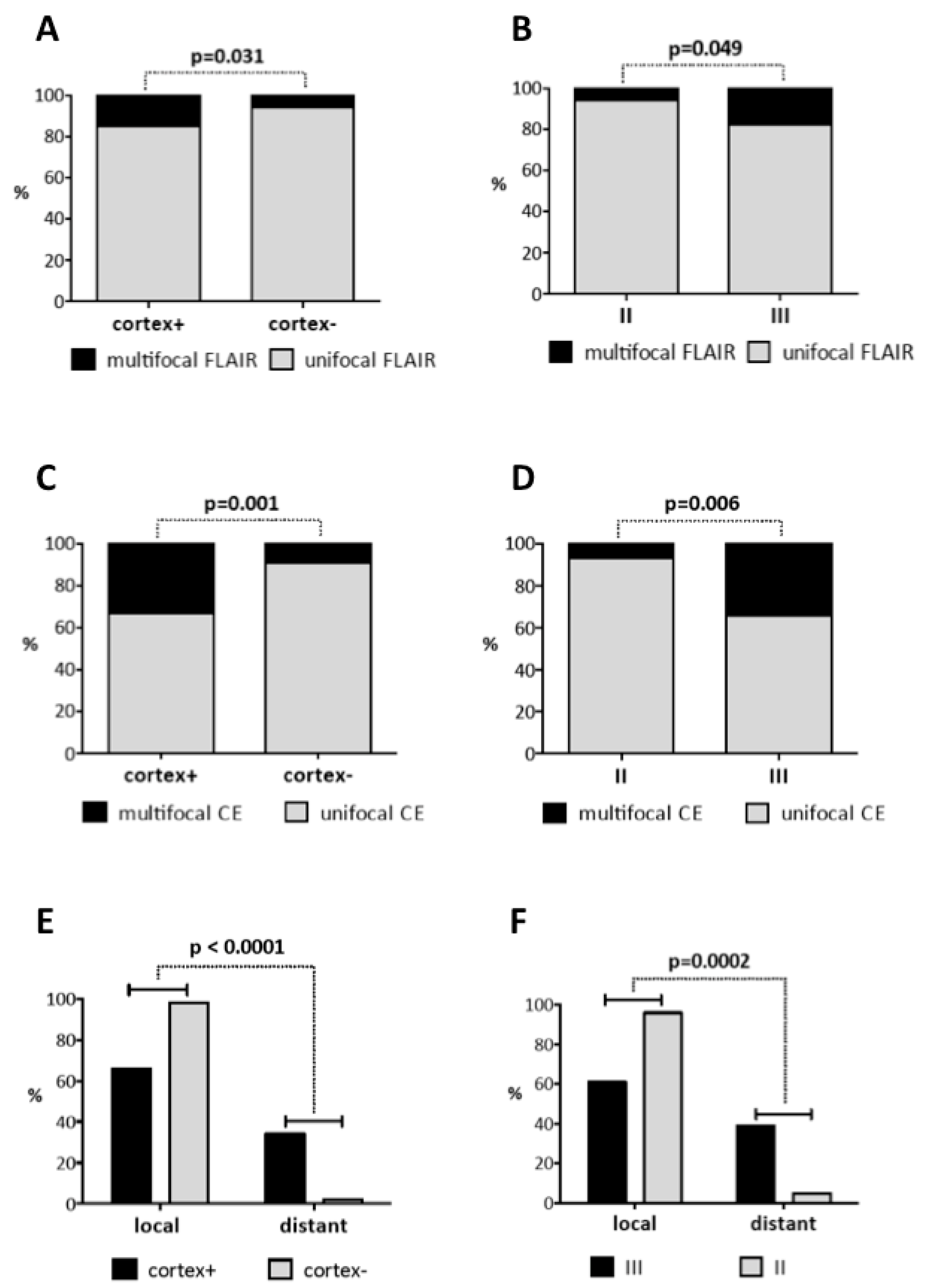
| Multifocal growth; n (%) - CE - FLAIR | 96 (100) 14 (15) 12 (13) | 53 (100) 4 (8) 3 (6) | 105 (100) 18 (17) 19 (18) | 31 (100) 2 (6) 2 (6) | 285 (100) 38 (13) 36 (13) | 0.235 0.100 | 0.602 0.212 | 0.056 0.031 | 0.146 0.049 |
| Radiographic Characteristics at Recurrence (n = 187) | |||||||||
| Imaging available; n (%) - Yes - No - Alive & no recurrence | 96 (100) 57 (59) 39 (41) 0 (0) | 53 (100) 28 (53) 25 (47) 0 (0) | 105 (100) 83 (79) 20 (19) 2 (2) | 31 (100) 19 (61) 11 (35) 1 (3) | 285 (100) 187 (66) 95 (33) 3 (1) | ||||
| Location at recurrence; n (%) - Group I (rec) - Group II (rec) - Group III (rec) - Group IV (rec) | 57 (100) 47 (82) 2 (3.5) 4 (7) 4 (7) | 28 (100) 16 (57) 9 (32) 2 (7) 1 (4) | 83 (100) 24 (29) 8 (9.5) 38 (46) 13 (15.5) | 19 (100) 3 (16) 5 (26) 6 (32) 5 (26) | 187 (100) 90 (48) 24 (13) 50 (27) 23 (12) | <0.0001 | <0.0001 | 0.0003 | <0.0001 |
| Recurrence pattern; n (%) - Local - Distant - Local & Distant | 57 (100) 41 (72) 3 (5) 13 (23) | 28 (100) 27 (96) 0 (0) 1 (4) | 83 (100) 51 (61) 8 (10) 24 (29) | 19 (100) 19 (100) 0 (0) 0 (0) | 187 (100) 138 (74) 11 (6) 38 (20) | 0.0001 | 0.078 | <0.0001 | 0.0002 |
| Multifocal growth; n (%) - Multifocal CE (rec) - Multifocal FLAIR (rec) | 57 (100) 18 (32) 7 (12) | 28 (100) 2 (7) 2 (7) | 83 (100) 28 (34) 18 (22) | 19 (100) 2 (11) 2 (11) | 187 (100) 50 (27) 29 (15.5) | 0.013 0.193 | 0.409 0.106 | 0.001 0.164 | 0.006 0.096 |
| Treatment at 1st Diagnosis (n = 285) | |||||||||
| EOR; n (%) - GTR - Partial - Biopsy - Unknown | 96 (100) 19 (20) 62 (64.5) 1 (1) 14 (14.5) | 53 (100) 10 (19) 30 (57) 6 (11) 7 (13) | 105 (100) 49 (47) 42 (40) 3 (3) 11 (10) | 31 (100) 14 (45) 15 (48) 0 (0) 2 (7) | 285 (100) 92 (32) 149 (52) 10 (4) 34 (12) | 0.0005 | <0.0001 | 0.556 | 0.003 |
| Adjuvant therapy; n (%) - RT - TMZ concomitant - Stupp - Clinical trial | 96 (100) 77 (80) 46 (48) 22 (23) 29 (30) | 53 (100) 44 (83) 34 (64) 12 (23) 17 (32) | 105 (100) 92 (88) 63 (60) 35 (33) 40 (38) | 31 (100) 27 (87) 19 (61) 10 (32) 8 (26) | 285 (100) 240 (84) 162 (57) 79 (28) 94 (33) | 0.289 0.509 | 0.064 0.451 | 0.773 0.492 | 0.199 0.488 |
| Treatment at Recurrence (n = 187) | |||||||||
| Salvage-therapy; n (%) - Treatment received - No treatment received - Lost to follow-up - Alive & no recurrence | 57 (100) 50 (88) 30 17 0 | 28 (100) 23 (82) 23 8 0 | 83 (100) 73 (88) 19 14 2 | 19 (100) 17 (89) 4 9 1 | 187 (100) 163 (87) 76 48 3 | 0.008 | 0.004 | 0.037 | 0.002 |
| Re-resection; n (%) - GTR - Partial - Unknown | 10 (20) 4 (8) 5 (10) 1 (2) | 5 (22) 2 (9) 2 (9) 0 | 24 (33) 15 (21) 5 (7) 1 (1) | 6 (35) 3 (18) 1 (6) 2 (12) | 45 (28) 24 (15) 13 (8) 4 (2) | 0.24 | 0.194 | 0.45 | 0.538 |
| Non-surgical therapies; n (%) - 0 (re-resection only) - 1 - 2–5 | 57 (100) 2 (4) 34 (68) 14 (28) | 28 (100) 1 (4) 13 (57) 9 (39) | 83 (100) 1 (1) 29 (40) 43 (59) | 19 (100) 0 5 (29) 12 (71) | 187 (100) 4 (2) 81 (50) 78 (48) | 0.013 | <0.001 | 0.789 | 0.209 |
| Clinical and Radiographic Factors | p-Value | HR | 95% CI |
|---|---|---|---|
| Overall Survival | |||
| SVZ+ (1st diagnosis) | 0.008 ** | 1.434 | 1.099–1.872 |
| Age (above median) | 0.036 * | 1.343 | 1.02–1.77 |
| KPS pre-operative | 0.110 | 0.993 | 0.985–1.002 |
| EOR: STR (1st diagnosis) | <0.0001 *** | 1.923 | 1.423–2.599 |
| Intensified Treatment (1st diagnosis) | <0.0001 *** | 0.302 | 0.221–0.412 |
| Multifocal disease CE (1st diagnosis) | 0.022 * | 1.56 | 1.067–2.280 |
| Progression-Free Survival | |||
| SVZ+ (1st diagnosis) | 0.529 | 0.918 | 0.703–1.199 |
| EOR: STR (1st diagnosis) | <0.0001 *** | 1.811 | 1.348–2.433 |
| Intensified Treatment (1st diagnosis) | <0.0001 *** | 0.431 | 0.322–0.579 |
| Multifocal disease FLAIR (1st diagnosis) | 0.013 * | 1.614 | 1.108–2.350 |
| Survival after Relapse | |||
| SVZ+ (at relapse) | 0.015 * | 1.575 | 1.092–2.273 |
| Cortex+ (at relapse) | <0.001 *** | 2.069 | 1.355–3.157 |
| Treatment Intensity (at relapse) | <0.001 *** | 0.768 | 0.67–0.88 |
| Multifocal disease FLAIR (at relapse) | 0.097 | 1.538 | 0.925–2.558 |
| Clinical and Radiographic Factors | p-Value | HR | 95% CI |
|---|---|---|---|
| Overall Survival | |||
| Location group II (1st diagnosis) | 0.007 * | 1.725 | 1.164–2.557 |
| Age (above median) | <0.0001 *** | 2.531 | 1.690–3.788 |
| KPS pre-operative | 0.139 | 1.009 | 0.997–1.021 |
| EOR: STR (1st diagnosis) | <0.001 *** | 2.15 | 1.452–3.184 |
| Intensified Treatment (1st diagnosis) | <0.0001 *** | 0.271 | 0.179–0.412 |
| Progression-Free Survival | |||
| Location group II (1st diagnosis) | 0.432 | 0.848 | 0.563–1.278 |
| EOR: STR (1st diagnosis) | 0.003 ** | 1.829 | 1.233–2.712 |
| Intensified Treatment (1st diagnosis) | <0.0001 *** | 0.406 | 0.270–0.611 |
| Multifocal disease FLAIR (1stdiagnosis) | 0.104 | 1.519 | 0.918–2.514 |
| Survival after Relapse | |||
| Location group II (at relapse) | 0.148 | 0.623 | 0.328–1.183 |
| Treatment Intensity (at relapse) | 0.002 ** | 0.702 | 0.560–0.879 |
| Multifocal disease FLAIR (at relapse) | 0.005 ** | 2.966 | 1.399–6.291 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jungk, C.; Warta, R.; Mock, A.; Friauf, S.; Hug, B.; Capper, D.; Abdollahi, A.; Debus, J.; Bendszus, M.; von Deimling, A.; et al. Location-Dependent Patient Outcome and Recurrence Patterns in IDH1-Wildtype Glioblastoma. Cancers 2019, 11, 122. https://doi.org/10.3390/cancers11010122
Jungk C, Warta R, Mock A, Friauf S, Hug B, Capper D, Abdollahi A, Debus J, Bendszus M, von Deimling A, et al. Location-Dependent Patient Outcome and Recurrence Patterns in IDH1-Wildtype Glioblastoma. Cancers. 2019; 11(1):122. https://doi.org/10.3390/cancers11010122
Chicago/Turabian StyleJungk, Christine, Rolf Warta, Andreas Mock, Sara Friauf, Bettina Hug, David Capper, Amir Abdollahi, Jürgen Debus, Martin Bendszus, Andreas von Deimling, and et al. 2019. "Location-Dependent Patient Outcome and Recurrence Patterns in IDH1-Wildtype Glioblastoma" Cancers 11, no. 1: 122. https://doi.org/10.3390/cancers11010122