Higher Screening Aldosterone to Renin Ratio in Primary Aldosteronism Patients with Diabetes Mellitus

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Subjects
2.3. Diagnosis and Further Lateralisation of PA
2.3.1. Confirmation
- autonomous excess aldosterone production evidenced with a 24-h urinary aldosterone level (Uald-24 h) more than 20.3 µg [14];
- TAIPAI score greater than 60% [16];
- post-saline loading plasma aldosterone concentration (PAC) > 10 ng/dL or PAC/PRA > 35 ng/dL per ng/mL/h shown in a post-captopril/losartan test or PAC > 6 ng/dL indicated by a fludrocortisone suppression test [7].
2.3.2. Subtype Identification
- adrenal adenoma evidenced with a CT scan for pre-operative evaluation; and
- lateralisation of aldosterone secretion at adrenal venous sampling (AVS) or during dexamethasone suppression NP-59 SPECT/CT [23]; and
- pathologically proven adenoma after an adrenalectomy for those who undergo surgery; and
- subsequent evidence of either a complete or partial cure of hypertension [24].
- evidence of bilateral diffuse adrenal enlargement indicated on CT scan; or
- non-lateralisation of aldosterone secretion at AVS or during dexamethasone suppression NP-59 SPECT/CT [23]; or
- evidence of diffuse adrenal cell hyperplasia reported in pathology studies for those undergoing surgery.
2.4. Definitions of General Parameters and Laboratory Data
2.5. Functional Survey
2.6. Statistical Analyses
3. Results
3.1. Clinical Characteristics of PA and EH Patients with DM or without DM
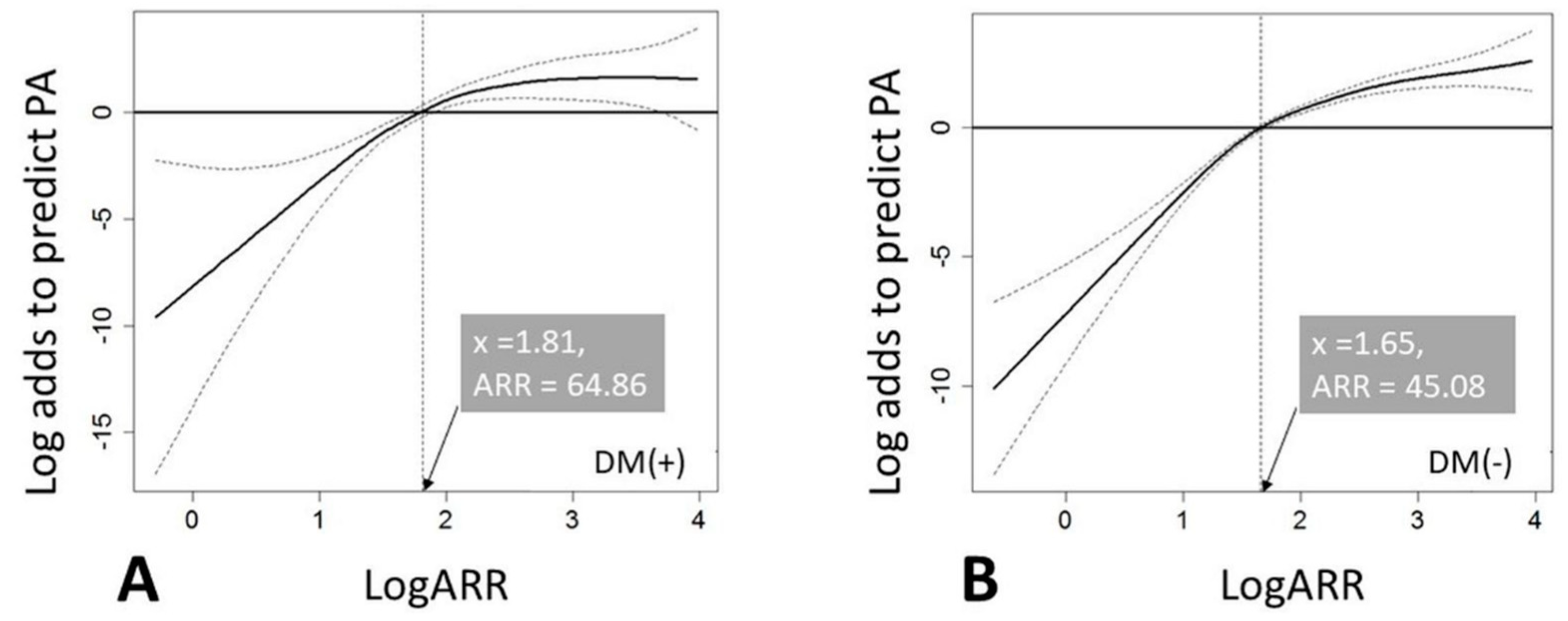
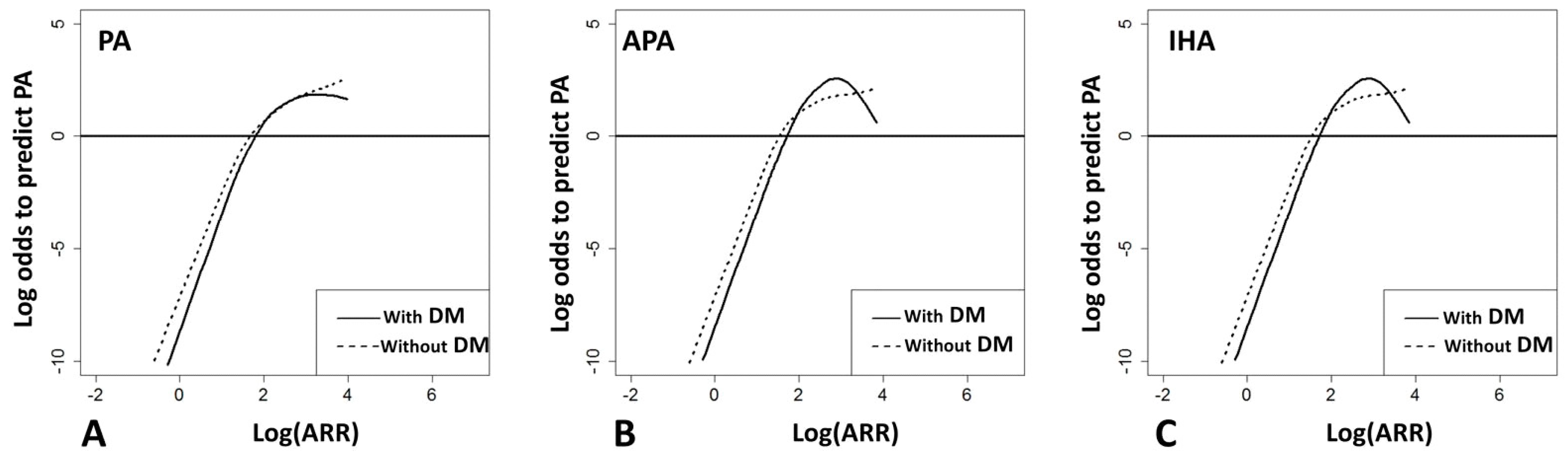
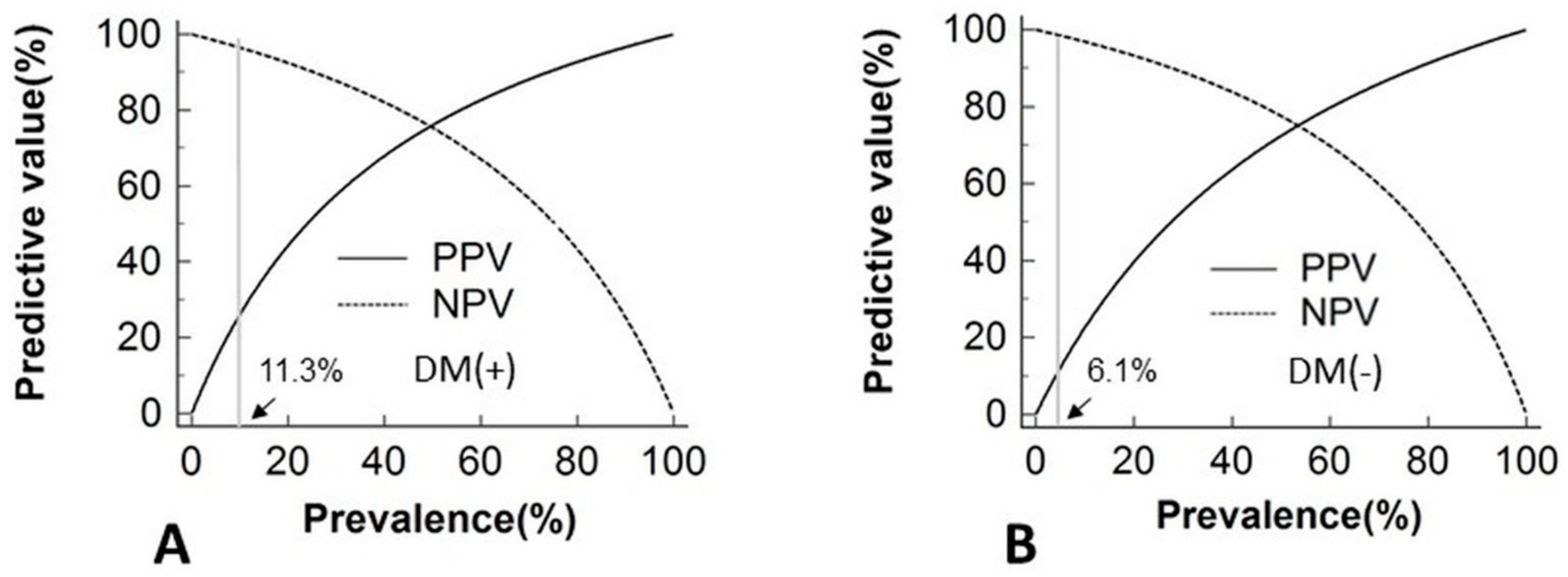
3.2. Effects of DM Status on ARR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Monticone, S.; Burrello, J.; Tizzani, D.; Bertello, C.; Viola, A.; Buffolo, F.; Gabetti, L.; Mengozzi, G.; Williams, T.A.; Rabbia, F.; et al. Prevalence and clinical manifestations of primary aldosteronism encountered in primary care practice. J. Am. Coll. Cardiol. 2017, 69, 1811–1820. [Google Scholar] [CrossRef] [PubMed]
- Funder, J.W.; Carey, R.M.; Mantero, F.; Murad, M.H.; Reincke, M.; Shibata, H.; Stowasser, M.; Young, W.F., Jr. The management of primary aldosteronism: Case detection, diagnosis, and treatment: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2016, 101, 1889–1916. [Google Scholar] [CrossRef] [PubMed]
- Muth, A.; Ragnarsson, O.; Johannsson, G.; Wangberg, B. Systematic review of surgery and outcomes in patients with primary aldosteronism. Br. J. Surg. 2015, 102, 307–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.H.; Lee, H.H.; Liu, K.L.; Lee, J.K.; Shih, S.R.; Chueh, S.C.; Lin, W.C.; Lin, L.C.; Lin, L.Y.; Chung, S.D.; et al. Reversal of myocardial fibrosis in patients with unilateral hyperaldosteronism receiving adrenalectomy. Surgery 2011, 150, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Wang, S.M.; Chang, C.H.; Hu, Y.H.; Lin, L.Y.; Lin, Y.H.; Chueh, S.C.; Chen, L.; Wu, K.D. Long term outcome of aldosteronism after target treatments. Sci. Rep. 2016, 6, 32103. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Wu, P.C.; Wu, C.H.; Huang, T.M.; Chang, C.H.; Tsai, P.R.; Ko, W.J.; Chen, L.; Wang, C.Y.; Chu, T.S.; et al. The impact of acute kidney injury on the long-term risk of stroke. J. Am. Heart Assoc. 2014, 3, e000933. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.T.; Wu, V.C.; Kuo, C.C.; Lin, Y.H.; Chang, C.C.; Chueh, S.J.; Wu, K.D.; Pimenta, E.; Stowasser, M. Diagnosis and management of primary aldosteronism: An updated review. Ann. Med. 2013, 45, 375–383. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation Guideline Development Group. Guideline for management of post-meal glucose in diabetes. Diabetes Res. Clin. Pract. 2014, 103, 256–268. [Google Scholar] [CrossRef] [PubMed]
- Reincke, M.; Meisinger, C.; Holle, R.; Quinkler, M.; Hahner, S.; Beuschlein, F.; Bidlingmaier, M.; Seissler, J.; Endres, S.; Participants of the German Conn’s Registry. Is primary aldosteronism associated with diabetes mellitus? Results of the German Conn’s Registry. Horm. Metab. Res. 2010, 42, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, J.J.; Khoo, C.M.; Thai, A.C.; Chionh, S.B.; Pin, L.; Lee, K.O. Type 2 diabetic patients with resistant hypertension should be screened for primary aldosteronism. Diabetes Vasc. Dis. Res. 2010, 7, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Umpierrez, G.E.; Cantey, P.; Smiley, D.; Palacio, A.; Temponi, D.; Luster, K.; Chapman, A. Primary aldosteronism in diabetic subjects with resistant hypertension. Diabetes Care 2007, 30, 1699–1703. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Cruz, A., Jr.; Noth, R.H.; Lassman, M.N.; Hollis, J.B.; Mulrow, P.J. Low plasma renin activity in normotensive patients with diabetes mellitus: Relationship to neuropathy. Hypertension 1981, 3, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, Z.; Moradi, M.; Nasri, H. A systematic review of the role of renin angiotensin aldosterone system genes in diabetes mellitus, diabetic retinopathy and diabetic neuropathy. J. Res. Med. Sci. 2014, 19, 1090–1098. [Google Scholar] [PubMed]
- Hsueh, W.A.; Wyne, K. Renin-angiotensin-aldosterone system in diabetes and hypertension. J. Clin. Hypertens. 2011, 13, 224–237. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Chueh, S.C.; Chang, H.W.; Lin, L.Y.; Liu, K.L.; Lin, Y.H.; Ho, Y.L.; Lin, W.C.; Wang, S.M.; Huang, K.H.; et al. Association of kidney function with residual hypertension after treatment of aldosterone-producing adenoma. Am. J. Kidney Dis. 2009, 54, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Yang, S.Y.; Lin, J.W.; Cheng, B.W.; Kuo, C.C.; Tsai, C.T.; Chu, T.S.; Huang, K.H.; Wang, S.M.; Lin, Y.H.; et al. Kidney impairment in primary aldosteronism. Clin. Chim. Acta 2011, 412, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Yang, Y.W.; Hu, Y.H.; Tsai, Y.C.; Kuo, K.L.; Lin, Y.H.; Hung, S.C.; Wu, V.C.; Wu, K.D.; Taiwan Primary Aldosteronism Investigation (TAIPAI) Study Group. Comparison of 24-h urinary aldosterone level and random urinary aldosterone-to-creatinine ratio in the diagnosis of primary aldosteronism. PLoS ONE 2013, 8, e67417. [Google Scholar]
- Wu, V.C.; Hu, Y.H.; Wu, C.H.; Kao, C.C.; Wang, C.Y.; Yang, W.S.; Lee, H.H.; Chang, Y.S.; Lin, Y.H.; Wang, S.M.; et al. Administrative data on diagnosis and mineralocorticoid receptor antagonist prescription identified patients with primary aldosteronism in Taiwan. J. Clin. Epidemiol. 2014, 67, 1139–1149. [Google Scholar] [CrossRef] [PubMed]
- Niizuma, S.; Nakahama, H.; Kamide, K.; Fukuchi, K.; Iwanaga, Y.; Nakata, H.; Yoshihara, F.; Horio, T.; Nakamura, S.; Kawano, Y. The cutoff value of aldosterone-to-renin ratio for the diagnosis of primary aldosteronism in patients taking antihypertensive medicine. Clin. Exp. Hypertens. 2008, 30, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.D.; Liao, T.S.; Chen, Y.M.; Lai, M.K.; Chen, S.J.; Su, C.T.; Chu, T.S.; Chang, C.C.; Hsieh, B.S. Preoperative diagnosis and localization of aldosterone-producing adenoma by adrenal venous sampling after administration of metoclopramide. J. Formos. Med. Assoc. 2001, 100, 598–603. [Google Scholar] [PubMed]
- Wu, V.C.; Huang, K.H.; Peng, K.Y.; Tsai, Y.C.; Wu, C.H.; Wang, S.M.; Yang, S.Y.; Lin, L.Y.; Chang, C.C.; Lin, Y.H.; et al. Prevalence and clinical correlates of somatic mutation in aldosterone producing adenoma-Taiwanese population. Sci. Rep. 2015, 5, 11396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.H.; Yang, Y.W.; Hung, S.C.; Tsai, Y.C.; Hu, Y.H.; Lin, Y.H.; Chu, T.S.; Wu, K.D.; Wu, V.C. Effect of treatment on body fluid in patients with unilateral aldosterone producing adenoma: Adrenalectomy versus spironolactone. Sci. Rep. 2015, 5, 15297. [Google Scholar] [CrossRef] [PubMed]
- Yen, R.F.; Wu, V.C.; Liu, K.L.; Cheng, M.F.; Wu, Y.W.; Chueh, S.C.; Lin, W.C.; Wu, K.D.; Tzen, K.Y.; Lu, C.C.; et al. 131I-6beta-iodomethyl-19-norcholesterol SPECT/CT for primary aldosteronism patients with inconclusive adrenal venous sampling and CT results. J. Nucl. Med. 2009, 50, 1631–1637. [Google Scholar] [CrossRef] [PubMed]
- Williams, T.A.; Lenders, J.W.M.; Mulatero, P.; Burrello, J.; Rottenkolber, M.; Adolf, C.; Satoh, F.; Amar, L.; Quinkler, M.; Deinum, J.; et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: An international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017, 5, 689–699. [Google Scholar] [CrossRef]
- Chiang, C.E.; Wang, T.D.; Ueng, K.C.; Lin, T.H.; Yeh, H.I.; Chen, C.Y.; Wu, Y.J.; Tsai, W.C.; Chao, T.H.; Chen, C.H.; et al. Guidelines of the Taiwan Society of Cardiology and the Taiwan Hypertension Society for the management of hypertension. J. Chin. Med. Assoc. 2015, 78, 1–47. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of medical care in diabetes-2015 abridged for primary care providers. Clin. Diabetes 2015, 33, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Hu, Y.H.; Tsai, Y.C.; Wu, C.H.; Wang, S.M.; Lin, L.Y.; Lin, Y.H.; Satoh, F.; Wu, K.D.; Wu, V.C. Arterial stiffness and blood pressure improvement in aldosterone-producing adenoma harboring KCNJ5 mutations after adrenalectomy. Oncotarget 2017, 8, 29984–29995. [Google Scholar] [CrossRef] [PubMed]
- Hin, L.Y.; Lau, T.K.; Rogers, M.S.; Chang, A.M. Dichotomization of continuous measurements using generalized additive modelling—Application in predicting intrapartum caesarean delivery. Stat. Med. 1999, 18, 1101–1110. [Google Scholar] [CrossRef]
- Yee, T.W. Quantile regression via vector generalized additive models. Stat. Med. 2004, 23, 2295–2315. [Google Scholar] [CrossRef] [PubMed]
- Murase, K.; Nagaishi, R.; Takenoshita, H.; Nomiyama, T.; Akehi, Y.; Yanase, T. Prevalence and clinical characteristics of primary aldosteronism in Japanese patients with type 2 diabetes mellitus and hypertension. Endocr. J. 2013, 60, 967–976. [Google Scholar] [CrossRef] [PubMed]
- Sousa, A.G.; Cabral, J.V.; El-Feghaly, W.B.; de Sousa, L.S.; Nunes, A.B. Hyporeninemic hypoaldosteronism and diabetes mellitus: Pathophysiology assumptions, clinical aspects and implications for management. World J. Diabetes 2016, 7, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.M.; Mehta, A.A. Aldosterone and angiotensin: Role in diabetes and cardiovascular diseases. Eur. J. Pharmacol. 2012, 697, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Luther, J.M.; Brown, N.J. The renin-angiotensin-aldosterone system and glucose homeostasis. Trends Pharmacol. Sci. 2011, 32, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Christlieb, A.R.; Kaldany, A.; D’Elia, J.A. Plasma renin activity and hypertension in diabetes mellitus. Diabetes 1976, 25, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Alderman, M.H.; Cohen, H.W.; Sealey, J.E.; Laragh, J.H. Plasma renin activity levels in hypertensive persons: Their wide range and lack of suppression in diabetic and in most elderly patients. Am. J. Hypertens. 2004, 17, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Nurulraziquin, M.J.; Suehazlyn, Z.; Amiliyatun, M. Aldosterone renin ratio (ARR) in recently diagnosed type 2 diabetes mellitus. J. Endocrinol. Metab. 2010, 1. [Google Scholar]
- Wu, V.C.; Chueh, S.J.; Chen, L.; Chang, C.H.; Hu, Y.H.; Lin, Y.H.; Wu, K.D.; Yang, W.S.; TAIPAI Study Group. Risk of new-onset diabetes mellitus in primary aldosteronism: A population study over 5 years. J. Hypertens. 2017, 35, 1698–1708. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Li, F.; He, C.; Zhu, Y.; Tan, W. Elevated prevalence of abnormal glucose metabolism in patients with primary aldosteronism: A meta-analysis. Irish J. Med. Sci. 2014, 183, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Rowe, J.W.; Tobin, J.D.; Rosa, R.M.; Andres, R. Effect of experimental potassium deficiency on glucose and insulin metabolism. Metabolism 1980, 29, 498–502. [Google Scholar] [CrossRef]
- Zillich, A.J.; Garg, J.; Basu, S.; Bakris, G.L.; Carter, B.L. Thiazide diuretics, potassium, and the development of diabetes: A quantitative review. Hypertension 2006, 48, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Bochud, M.; Nussberger, J.; Bovet, P.; Maillard, M.R.; Elston, R.C.; Paccaud, F.; Shamlaye, C.; Burnier, M. Plasma aldosterone is independently associated with the metabolic syndrome. Hypertension 2006, 48, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Ares-Carrasco, S.; Picatoste, B.; Benito-Martín, A.; Zubiri, I.; Sanz, A.B.; Sánchez-Niño, M.D.; Ortiz, A.; Egido, J.; Tuñón, J.; Lorenzo, O. Myocardial fibrosis and apoptosis, but not inflammation, are present in long-term experimental diabetes. Am. J. Physiol. Heart. Circ. Physiol. 2009, 297, 2109–2119. [Google Scholar] [CrossRef] [PubMed]
- Fiordaliso, F.; De Angelis, N.; Bai, A.; Cuccovillo, I.; Salio, M.; Serra, D.M.; Bianchi, R.; Razzetti, R.; Latini, R.; Masson, S. Effect of beta-adrenergic and renin-angiotensin system blockade on myocyte apoptosis and oxidative stress in diabetic hypertensive rats. Life Sci. 2007, 81, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Pan, Z.Q.; Xie, D.; Choudhary, V.; Seremwe, M.; Tsai, Y.Y.; Olala, L.; Chen, X.; Bollag, W.B. The effect of pioglitazone on aldosterone and cortisol production in HAC15 human adrenocortical carcinoma cells. Mol. Cell. Endocrinol. 2014, 394, 119–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skov, J.; Dejgaard, A.; Frøkiær, J.; Holst, J.J.; Jonassen, T.; Rittig, S.; Christiansen, J.S. Glucagon-like peptide-1 (GLP-1): Effect on kidney hemodynamics and renin-angiotensin-aldosterone system in healthy men. J. Clin. Endocrinol. Metab. 2013, 98, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, P.; Aggarwal, R. Common pitfalls in statistical analysis: Understanding the properties of diagnostic tests—Part 1. Perspect. Clin. Res. 2018, 9, 40–43. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| General Parameters | Total, n = 844 | DM (+), n = 136 | DM (−), n = 708 | p Value |
|---|---|---|---|---|
| Female (%) | 455 (54) | 58 (43) | 395 (56) | 0.010 * |
| BMI (kg/m2) | 25.5 ± 4.1 | 26.7 ± 4.4 | 25.3 ± 4.0 | <0.001 † |
| Duration of HTN (years) | 8.2 ± 7.8 | 10.9 ± 9.2 | 7.7 ± 7.4 | <0.001 † |
| SBP (mmHg) | 149 ± 22 | 155 ± 22 | 148 ± 21 | <0.001 † |
| DBP (mmHg) | 89 ± 14 | 90 ± 14 | 88 ± 14 | 0.196 |
| HR (beats) | 74 ± 12 | 74 ± 12 | 74 ± 12 | 0.673 |
| Anti-hypertensive drugs (number) | 2.3 ± 1.1 | 2.5 ± 1.2 | 2.3 ± 1.0 | 0.016 * |
| Baseline comorbidities | ||||
| CVA (%) | 49 (6) | 12 (9) | 37 (5) | 0.103 |
| LVH (%) | 128 (15) | 21 (15) | 107 (15) | 0.917 |
| CAD (%) | 94 (11) | 40 (29) | 54 (8) | <0.001 † |
| Laboratory data at screening period | ||||
| PAC (ng/dL) | 55.5 ± 62.7 | 50.4 ± 33.3 | 56.5 ± 66.8 | 0.300 |
| PRA (ng/mL/h) | 0.53 ± 0.77 | 0.45 ± 0.55 | 0.55 ± 0.81 | 0.183 |
| ARR (ng/dL per ng/mL/h) | 610.9 ± 1332.7 | 678.9 ± 1510.0 | 597.8 ± 1296.7 | 0.516 |
| eGFR (mL/min/1.73 m2) | 84.5 ± 24.5 | 74.5 ± 26.9 | 86.5 ± 23.6 | <0.001 † |
| Serum potassium (mmol/L) | 3.6 ± 0.7 | 3.6 ± 0.7 | 3.6 ± 0.7 | 0.897 |
| 24-h urinary aldosterone (μg/day) | 20.2 ± 7.3 | 19.9 ± 8.3 | 20.3 ± 7.1 | 0.683 |
| General Parameters | Total, n = 225 | PA (+), n = 136 | PA (−), n = 89 | p Value |
|---|---|---|---|---|
| Age( years) | 56.7 ± 12.3 | 56.1 ± 12.3 | 57.5 ± 12.3 | 0.387 |
| Female (%) | 96 (43) | 58 (43) | 38 (43) | 0.994 |
| BMI (kg/m2) | 26.6 ± 4.2 | 26.7 ± 4.4 | 26.6 ± 3.9 | 0.884 |
| Duration of HTN (years) | 10.1 ± 8.8 | 10.9 ± 9.2 | 8.9 ± 8.2 | 0.034 * |
| SBP (mmHg) | 155 ± 21 | 155 ± 20 | 154 ± 21 | 0.994 |
| DBP (mmHg) | 91 ± 14 | 92 ± 14 | 91 ± 15 | 0.528 |
| HR (beats/min) | 74 ± 11 | 74 ± 12 | 75 ± 12 | 0.494 |
| Anti-hypertensive drugs (number) | 2.5 ± 1.2 | 2.6 ± 1.2 | 2.5 ± 1.1 | 0.705 |
| Baseline comorbidities | ||||
| CVA (%) | 19 (8) | 12 (9) | 7 (8) | 0.805 |
| LVH (%) | 28 (12) | 21 (15) | 7 (8) | 0.100 |
| CAD (%) | 65 (29) | 40 (29) | 25 (28) | 0.832 |
| Laboratory data at screening | ||||
| PAC (ng/dL) | 44.0 ±2 9.5 | 50.4 ± 33.3 | 34.1 ± 18.8 | <0.001 † |
| PRA (ng/mL/h) | 2.0 ± 6.3 | 0.5 ± 0.6 | 4.4 ± 9.5 | <0.001 † |
| ARR (ng/dL per ng/mL/h) | 474.6 ± 1296.2 | 678.9 ± 1510.0 | 162.3 ± 784.6 | <0.001 † |
| eGFR (mL/min/1.73 m2) | 73.4 ± 27.7 | 74.5 ± 26.9 | 71.6 ± 28.9 | 0.453 |
| Serum potassium (mmol/L) | 3.8 ± 0.7 | 3.6 ± 0.7 | 4.2 ± 0.5 | <0.001 † |
| 24-h urinary aldosterone (μg/day) | 16.3 ± 7.5 | 19.9 ± 8.3 | 10.8 ± 6.2 | <0.001 † |
| General Parameters | PA (+), n = 136 | PA (−), n = 89 | Odds Ratio | 95% CI | p Value |
|---|---|---|---|---|---|
| Age (years) | 56.1 ± 12.3 | 57.5 ± 12.3 | |||
| Female (%) | 58 (43) | 38 (43) | |||
| BMI (kg/m2) | 26.7 ± 4.4 | 26.6 ± 3.9 | |||
| Duration of HTN (years) | 10.9 ± 9.2 | 8.9 ± 8.2 | |||
| SBP (mmHg) | 155 ± 20 | 154 ± 21 | |||
| DBP (mmHg) | 92 ± 14 | 91 ± 15 | |||
| HR (beats/min) | 74 ± 12 | 75 ± 12 | |||
| Anti-hypertensive drugs (number) | 2.6 ± 1.2 | 2.5 ± 1.1 | |||
| Baseline comorbidities | |||||
| CVA (%) | 12 (9) | 7 (8) | |||
| LVH (%) | 21 (15) | 7 (8) | |||
| CAD (%) | 40 (29) | 25 (28) | |||
| Preoperative laboratory data | |||||
| PAC (ng/dL) | 50.4 ± 33.3 | 34.1 ± 18.8 | 1.040 | 1.018–1.062 | <0.001 † |
| PRA (ng/mL/h) | 0.45 ± 0.55 | 4.4 ± 9.5 | 0.233 | 0.125–0.432 | <0.001 † |
| eGFR (mL/min/1.73 m2) | 74.5 ± 26.9 | 71.6 ± 28.9 | |||
| Serum potassium (mmol/L) | 3.6 ± 0.7 | 4.2 ± 0.5 | 0.196 | 0.098–0.394 | <0.001 † |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-H.; Hu, Y.-H.; Huang, K.-H.; Lin, Y.-H.; Tsai, Y.-C.; Wu, C.-H.; Yang, S.-Y.; Chang, C.-C.; Lu, C.-C.; Wu, K.-D.; et al. Higher Screening Aldosterone to Renin Ratio in Primary Aldosteronism Patients with Diabetes Mellitus. J. Clin. Med. 2018, 7, 360. https://doi.org/10.3390/jcm7100360
Chang C-H, Hu Y-H, Huang K-H, Lin Y-H, Tsai Y-C, Wu C-H, Yang S-Y, Chang C-C, Lu C-C, Wu K-D, et al. Higher Screening Aldosterone to Renin Ratio in Primary Aldosteronism Patients with Diabetes Mellitus. Journal of Clinical Medicine. 2018; 7(10):360. https://doi.org/10.3390/jcm7100360
Chicago/Turabian StyleChang, Chia-Hui, Ya-Hui Hu, Kuo-How Huang, Yen-Hung Lin, Yao-Chou Tsai, Che-Hsiung Wu, Shao-Yu Yang, Chin-Chen Chang, Ching-Chu Lu, Kwan-Dun Wu, and et al. 2018. "Higher Screening Aldosterone to Renin Ratio in Primary Aldosteronism Patients with Diabetes Mellitus" Journal of Clinical Medicine 7, no. 10: 360. https://doi.org/10.3390/jcm7100360