The Role of Objectively Measured, Altered Physical Activity Patterns for Body Mass Index Change during Inpatient Treatment in Female Patients with Anorexia Nervosa

 , ,
, ,
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Population
2.2. Anthropometry
2.3. Bioelectrical Impedance Analysis
2.4. PA Assessment
- A MET-value ≤1.0 was defined as the rate of energy expenditure while at rest [17].
- Activities with a MET-value ≤1.8 were considered as sedentary behavior [18].
- Thus, we concluded to form a new category ranging from ≥1.1 to ≤1.8 METs to describe very light-intensity physical activities (VLPA).
- Light-intensity physical activities (LPA) were defined as MET-values >1.8 and <3 [18].
- Vigorous-intensity activities (VPA) were divided firstly into MET-values ranging from ≥6 to ≤9, and secondly into values >9 METs [3].
2.5. Statistical Analysis
3. Results
3.1. Characterization of the Study Population Including Medical Details, Comorbidities, Medications, and Body Composition
3.2. Comparison of Physical Activity and MET Intensities
3.3. BMI Change
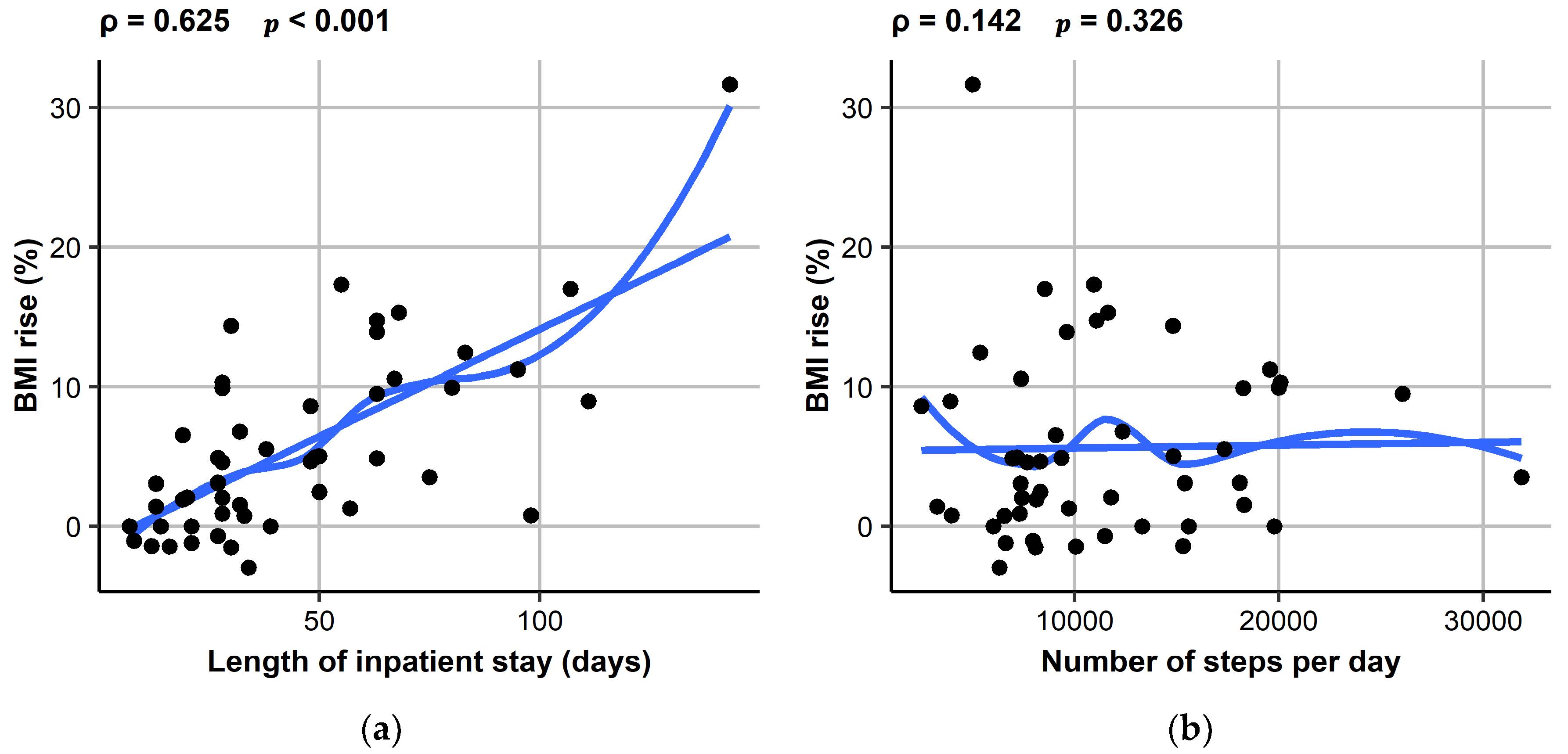
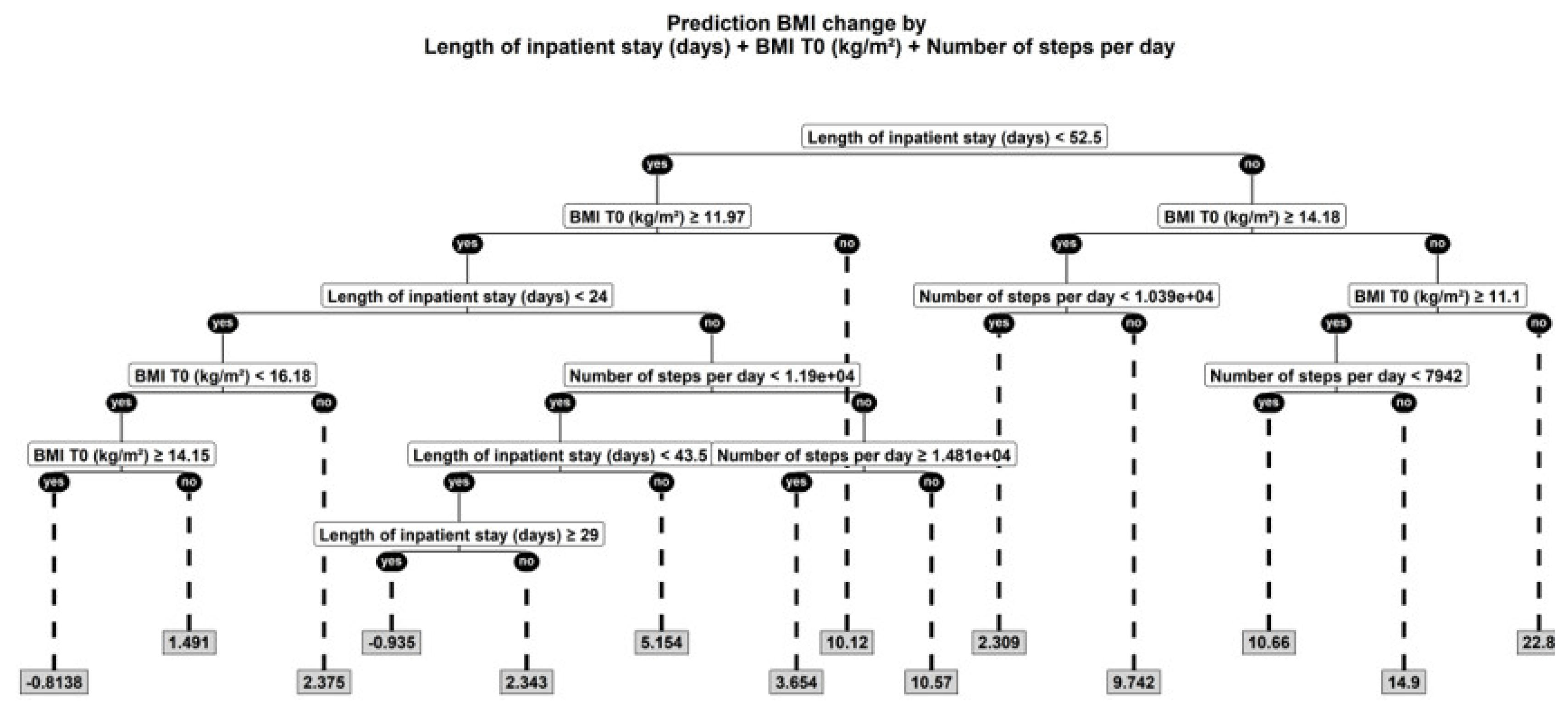
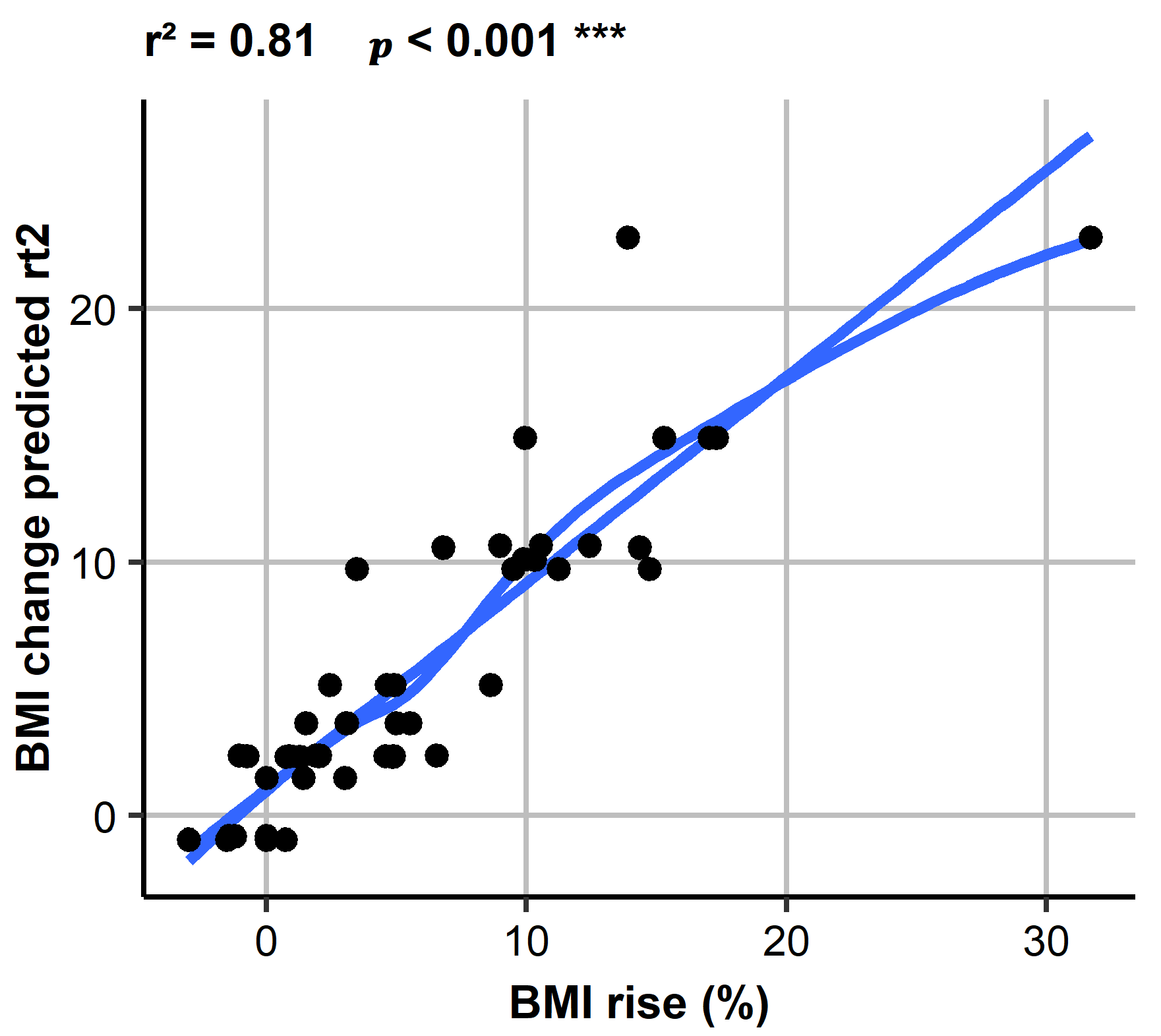
3.4. Association between Physical Activity and Clinical Outcome
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Solenberger, S.E. Exercise and eating disorders: A 3-year inpatient hospital record analysis. Eat. Behav. 2001, 2, 151–168. [Google Scholar] [CrossRef]
- Strober, M.; Freeman, R.; Morrell, W. The long-term course of severe anorexia nervosa in adolescents: Survival analysis of recovery, relapse, and outcome predictors over 10–15 years in a prospective study. Int. J. Eat. Disord. 1997, 22, 339–360. [Google Scholar] [CrossRef]
- El Ghoch, M.; Calugi, S.; Pellegrini, M.; Milanese, C.; Busacchi, M.; Battistini, N.C.; Bernabè, J.; Dalle Grave, R. Measured physical activity in anorexia nervosa: Features and treatment outcome. Int. J. Eat. Disord. 2013, 46, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Carrera, O.; Adan, R.A.; Gutierrez, E.; Danner, U.N.; Hoek, H.W.; van Elburg, A.A.; Kas, M.J. Hyperactivity in anorexia nervosa: Warming up not just burning-off calories. PLoS ONE 2012, 7, e41851. [Google Scholar] [CrossRef] [PubMed]
- Gümmer, R.; Giel, K.E.; Schag, K.; Resmark, G.; Junne, F.P.; Becker, S.; Zipfel, S.; Teufel, M. High levels of physical activity in anorexia nervosa: A systematic review. Eur. Eat. Disord. Rev. 2015, 23, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Kostrzewa, E.; van Elburg, A.A.; Sanders, N.; Sternheim, L.; Adan, R.A.; Kas, M.J. Longitudinal changes in the physical activity of adolescents with anorexia nervosa and their influence on body composition and leptin serum levels after recovery. PLoS ONE 2013, 8, e78251. [Google Scholar] [CrossRef] [PubMed]
- Rizk, M.; Lalanne, C.; Berthoz, S.; Kern, L.; EVHAN Group; Godart, N. Problematic exercise in anorexia nervosa: Testing potential risk factors against different definitions. PLoS ONE 2015, 10, e0143352. [Google Scholar] [CrossRef] [PubMed]
- Gianini, L.M.; Klein, D.A.; Call, C.; Walsh, B.T.; Wang, Y.; Wu, P.; Attia, E. Physical activity and post-treatment weight trajectory in anorexia nervosa. Int. J. Eat. Disord. 2016, 49, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Keyes, A.; Woerwag-Mehta, S.; Bartholdy, S.; Koskina, A.; Middleton, B.; Connan, F.; Webster, P.; Schmidt, U.; Campbell, I.C. Physical activity and the drive to exercise in anorexia nervosa. Int. J. Eat. Disord. 2015, 48, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Sauchelli, S.; Arcelus, J.; Sánchez, I.; Riesco, N.; Jiménez-Murcia, S.; Granero, R.; Gunnard, K.; Baños, R.; Botella, C.; de la Torre, R.; et al. Physical activity in anorexia nervosa: How relevant is it to therapy response? Eur. Psychiatry 2015, 30, 924–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belak, L.; Gianini, L.; Klein, D.A.; Sazonov, E.; Keegan, K.; Neustadt, E.; Walsh, B.T.; Attia, E. Measurement of fidgeting in patients with anorexia nervosa using a novel shoe-based monitor. Eat. Behav. 2017, 24, 45–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stengel, A.; Haas, V.; Elbelt, U.; Correll, C.U.; Rose, M.; Hofmann, T. Leptin and physical activity in adult patients with anorexia nervosa: Failure to demonstrate a simple linear association. Nutrients 2017, 9, 1210. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, T.; Elbelt, U.; Ahnis, A.; Kobelt, P.; Rose, M.; Stengel, A. Irisin levels are not affected by physical activity in patients with anorexia nervosa. Front. Endocrinol. (Lausanne) 2014, 4, 202. [Google Scholar] [CrossRef] [PubMed]
- Andre, D.; Pelletier, R.; Farringdon, J.; Safier, S.; Talbott, W.; Stone, R.; Vyas, N.; Trimble, J.; Wolf, D.; Vishnubhatla, S.; et al. The Development of the SenseWear® Armband, a Revolutionary Energy Assessment Device to Assess Physical Activity and Lifestyle. BodyMedia Inc., 2006. Available online: http://1fw.dotfit.com/sites/63/templates/categories/images/1783/Dev_SenseWear_article.pdf (accessed on 23 August 2018).
- Das Armband Kompendium. Available online: http://www.body-coaches.de/wp-content/uploads/Armband_Anleitung.pdf (accessed on 23 August 2018).
- Gastin, P.B.; Cayzer, C.; Dwyer, D.; Robertson, S. Validity of the ActiGraph GT3X+ and BodyMedia SenseWear Armband to estimate energy expenditure during physical activity and sport. J. Sci. Med. Sport 2018, 21, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines for Americans; US Department of Health and Human Services: Washington, DC, USA, 2008; pp. 15–34.
- Scheers, T.; Philippaerts, R.; Lefevre, J. Patterns of physical activity and sedentary behavior in normal-weight, overweight and obese adults, as measured with a portable armband device and an electronic diary. Clin. Nutr. 2012, 31, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Sternheim, L.; Danner, U.; Adan, R.; van Elburg, A. Drive for activity in patients with anorexia nervosa. Int. J. Eat. Disord. 2015, 48, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Adan, R.A.; Hillebrand, J.J.; Danner, U.N.; Cardona Cano, S.; Kas, M.J.; Verhagen, L.A. Neurobiology driving hyperactivity in activity-based anorexia. Curr. Top. Behav. Neurosci. 2011, 6, 229–250. [Google Scholar] [PubMed]
- Casper, R.C. Restless activation and drive for activity in anorexia nervosa may reflect a disorder of energy homeostasis. Int. J. Eat. Disord. 2016, 49, 750–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bratland-Sanda, S.; Sundgot-Borgen, J.; Rø, Ø.; Rosenvinge, J.H.; Hoffart, A.; Martinsen, E.W. Physical activity and exercise dependence during inpatient treatment of longstanding eating disorders: An exploratory study of excessive and non-excessive exercisers. Int. J. Eat. Disord. 2010, 43, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Eckert, E.D.; Gottesman, I.I.; Swigart, S.E.; Casper, R.C. A 57-year follow-up investigation and review of the Minnesota study on human starvation and its relevance to eating disorders. Arch. Psychol. 2018, 2, 3. [Google Scholar]
- Ravussin, E.; Lillioja, S.; Anderson, T.E.; Christin, L.; Bogardus, C. Determinants of 24-hour energy expenditure in man. Methods and results using a respiratory chamber. J. Clin. Investig. 1986, 78, 1568–1578. [Google Scholar] [CrossRef] [PubMed]
- Garland, T., Jr.; Schutz, H.; Chappell, M.A.; Keeney, B.K.; Meek, T.H.; Copes, L.E.; Acosta, W.; Drenowatz, C.; Maciel, R.C.; van Dijk, G.; et al. The biological control of voluntary exercise, spontaneous physical activity and daily energy expenditure in relation to obesity: Human and rodent perspectives. J. Exp. Biol. 2011, 214, 206–229. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.A.; Eberhardt, N.L.; Jensen, M.D. Role of nonexercise activity thermogenesis in resistance to fat gain in humans. Science 1999, 283, 212–214. [Google Scholar] [CrossRef] [PubMed]
- Haas, V.; Stengel, A.; Mähler, A.; Gerlach, G.; Lehmann, C.; Boschmann, M.; de Zwaan, M.; Herpertz, S. Metabolic barriers to weight gain in patients with anorexia nervosa: A young adult case report. Front. Psychiatry 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Calogero, R.M.; Pedrotty, K.N. The practice and process of healthy exercise: An investigation of the treatment of exercise abuse in women with eating disorders. Eat. Disord. 2004, 12, 273–291. [Google Scholar] [CrossRef] [PubMed]
- Haas, V.K.; Gaskin, K.J.; Kohn, M.R.; Clarke, S.D.; Müller, M.J. Different thermic effects of leptin in adolescent females with varying body fat content. Clin. Nutr. 2010, 29, 639–645. [Google Scholar] [CrossRef] [PubMed]
- El Ghoch, M.; Calugi, S.; Pellegrini, M.; Chignola, E.; Dalle Grave, R. Physical activity, body weight, and resumption of menses in anorexia nervosa. Psychiatry Res. 2016, 246, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Hagman, J.; Pan, Z.; MacLean, P. Increased physical activity not decreased energy intake is associated with inpatient medical treatment for anorexia nervosa in adolescent females. PLoS ONE 2013, 8, e61559. [Google Scholar] [CrossRef] [PubMed]
- Delvenne, V.; Kerkhofs, M.; Appelboom-Fondu, J.; Lucas, F.; Mendlewicz, J. Sleep polygraphic variables in anorexia nervosa and depression: A comparative study in adolescents. J. Affect. Disord. 1992, 25, 167–172. [Google Scholar] [CrossRef]
- El Ghoch, M.; Calugi, S.; Bernabè, J.; Pellegrini, M.; Milanese, C.; Chignola, E.; Dalle Grave, R. Sleep patterns before and after weight restoration in females with anorexia nervosa: A longitudinal controlled study. Eur. Eat. Disord. Rev. 2016, 24, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhai, L.; Zhang, D. Sleep duration and obesity among adults: A meta-analysis of prospective studies. Sleep Med. 2014, 15, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Taggart, F.M.; Kandala, N.B.; Currie, A.; Peile, E.; Stranges, S.; Miller, M.A. Meta-analysis of short sleep duration and obesity in children and adults. Sleep 2008, 31, 619–626. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Measurement Parameters | Anorexia Nervosa Baseline (n = 50) | Controls (n = 30) | p |
|---|---|---|---|
| Demographic parameters | |||
| Age (years) | 25 (21/30) | 26 (23/35) | 0.057 |
| Weight (kg) | 39.9 ± 6.6 (28.4–58.8) | 60.5 ± 5.8 (51.2–71.9) | <0.001 |
| Height (cm) | 166 ± 7 (152–185) | 169 ± 6 (159–180) | 0.128 |
| BMI (kg/m2) | 14.4 ± 2.0 (8.9–17.7) | 21.3 ± 1.7 (18.8–25.0) | <0.001 |
| Duration of illness (months) | 72 (15/134) | N/A | |
| Body composition | |||
| Phase angle (°) | 4.5 (3.8/5.1) | 5.9 (5.5/6.4) | <0.001 |
| Fat mass (kg) | 2.9 ± 2.7 (1–12.5) | 16.0 ± 3.1 (11.3–22.5) | <0.001 |
| Fat mass (%) | 6.7 ± 5.2 (2.1–21.6) | 26 ± 3 (21–32) | <0.001 |
| Fat-free mass (kg) | 37 ± 4 (27–46) | 44 ± 3 (39–53) | <0.001 |
| Fat-free mass (%) | 93 ± 5 (78–98) | 74 ± 3 (68–79) | <0.001 |
| Measurement Parameters | Anorexia Nervosa Baseline (n = 50) | Controls (n = 30) | p |
|---|---|---|---|
| Physical activity | |||
| Number of steps per day | 11,305 ± 6064 (2479–31,876) | 11,098 ± 3973 (6507–22,948) | 0.854 |
| Total distance (km/day) | 10.2 ± 5.5 (2.3–25.2) | 9.8 ± 4.0 (4.6–19.2) | 0.769 |
| Metabolic equivalents (METs per day) | 1.40 (1.40/1.60) | 1.70 (1.50/1.80) | <0.001 |
| Duration of recumbency (min/day) | 483 (443/527) | 500 (440/560) | 0.348 |
| Duration of sleep (min/day) | 427 (375/457) | 408 (363/484) | 0.842 |
| PA ≤ 1 METs duration (min/day) | 496 (448/536) | 588 (502/643) | <0.001 |
| VLPA 1.1–1.8 METs duration (min/day) | 647 (569/703) | 566 (499/631) | 0.004 |
| LPA 1.8–3 METs duration (min/day) | 126 (92/188) | 84 (71/108) | <0.001 |
| MPA 3–6 METs duration (min/day) | 82 (44/130) | 114 (79/165) | 0.022 |
| VPA 6–9 METs duration (min/day) | 0 (0/3) | 16 (8/35) | <0.001 |
| VPA > 9 METs duration (min/day) | 0.0 (0.0/0.0) | 0.0 (0.0/3.2) | 0.063 |
| Measurement Parameters | Anorexia Nervosa Baseline (n = 50) | Anorexia Nervosa Discharge (n = 50) | p |
|---|---|---|---|
| Clinical outcome | |||
| Weight (kg) | 39.9 ± 6.6 (28.4–58.8) | 42.0 ± 6.2 (31.4–59.7) | <0.001 |
| Total weight gain (kg) | - | 2.1 ± 2.3 (−1.4–9.6) | |
| BMI (kg/m2) | 14.4 ± 2.0 (8.9–17.7) | 15.2 ± 1.8 (11.7–18.3) | <0.001 |
| BMI increase (kg/ m2) | - | 0.7 ± 0.8 (−0.5–2.8) | |
| BMI increase (%) | - | 4 (1/10) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehmann, C.S.; Hofmann, T.; Elbelt, U.; Rose, M.; Correll, C.U.; Stengel, A.; Haas, V. The Role of Objectively Measured, Altered Physical Activity Patterns for Body Mass Index Change during Inpatient Treatment in Female Patients with Anorexia Nervosa. J. Clin. Med. 2018, 7, 289. https://doi.org/10.3390/jcm7090289
Lehmann CS, Hofmann T, Elbelt U, Rose M, Correll CU, Stengel A, Haas V. The Role of Objectively Measured, Altered Physical Activity Patterns for Body Mass Index Change during Inpatient Treatment in Female Patients with Anorexia Nervosa. Journal of Clinical Medicine. 2018; 7(9):289. https://doi.org/10.3390/jcm7090289
Chicago/Turabian StyleLehmann, Celine S., Tobias Hofmann, Ulf Elbelt, Matthias Rose, Christoph U. Correll, Andreas Stengel, and Verena Haas. 2018. "The Role of Objectively Measured, Altered Physical Activity Patterns for Body Mass Index Change during Inpatient Treatment in Female Patients with Anorexia Nervosa" Journal of Clinical Medicine 7, no. 9: 289. https://doi.org/10.3390/jcm7090289